Androgen therapy in women: a path to be more travelled?

Sexual problems in women
Androgens exert important effects on numerous biological events in women, being the obligatory precursors for oestrogen synthesis. Androgens have been used for decades, but when should testosterone therapy be prescribed for women and how should these patients be monitored?
- The main circulating androgenic steroids are dehydroepiandrosterone (DHEA), androstenedione and testosterone.
- DHEA and androstenedione are considered androgen precursors with little androgenic activity.
- Testosterone is a bioactive androgen converted within the peripheral target tissues and cells into dihydrotestosterone.
- The only indication for testosterone therapy supported by evidence is the management of hypoactive sexual desire dysfunction in postmenopausal women.
- During short-term testosterone use in postmenopausal women, no severe adverse events have been demonstrated when testosterone levels achieved are similar to physiological testosterone concentrations for premenopausal women.
- Regulatory approved women’s formulations of testosterone are essential and urgently needed to ensure safety and enable research into long-term use.
Testosterone therapy has been shown to improve low sexual desire associated with distress in postmenopausal women. This article reviews the physiology of testosterone in women, indications for testosterone therapy and treatment options for women with low sexual desire.
Testosterone physiology in women
Androgens are responsible for male secondary sexual characteristics; however, these hormones are crucial for a number of physiological events in women including normal ovarian follicular development, bone and muscle health, and vascular endothelial and sexual function.1
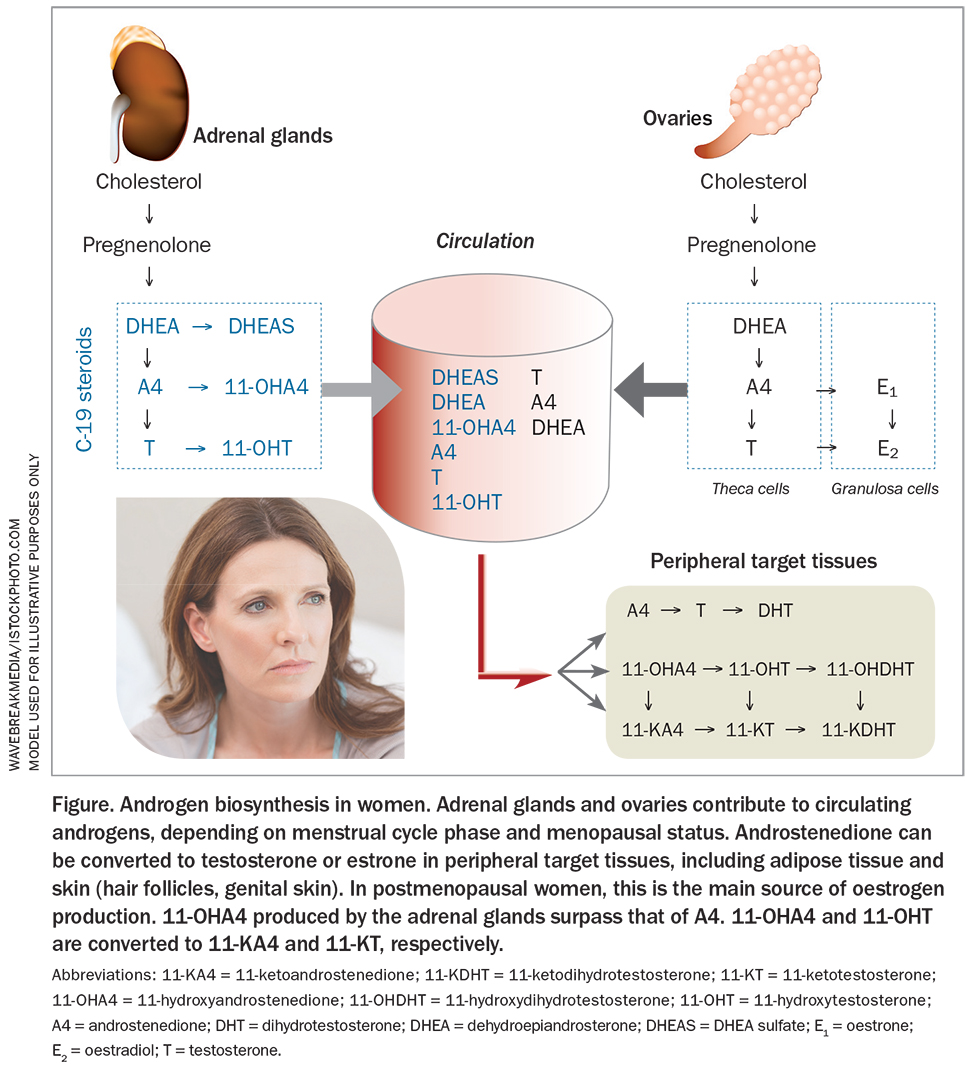
The main circulating androgen is testosterone. Dehydroepiandrosterone (DHEA) and androstenedione, which share a 19-carbon structure with testosterone (all called C-19 steroids), are considered androgen precursors with little androgenic activity. Testosterone is a bioactive androgen that is also converted within peripheral target tissues and cells into dihydrotestosterone (DHT), the most potent androgen available.
The adrenal glands are the main source of the testosterone precursors DHEA and its sulfate, DHEAS. Although circulating DHEAS is mainly of adrenal origin, androstenedione is secreted by the adrenals and ovaries. These adrenal and ovarian androgen precursors are secreted into the circulation and then activated in peripheral target tissues by their own intracellular steroidogenic enzymes to meet the physiological needs of local tissue (Figure).
{kind=link}
Most testosterone circulates bound to sex hormone-binding globulin (SHBG; 66%), and nearly a third to albumin and other plasma protein. About 1 to 2% of testosterone circulates without binding to any protein and is called free testosterone. Factors that increase SHBG levels result in lower free testosterone and, in turn, lower SHBG levels will increase free testosterone levels. Until recently, free testosterone was believed to be the bioactive hormone fraction but it was proposed that free testosterone could be instead the fraction available for rapid degradation.2 When free testosterone levels are reported, they have been inconsistent, estimated by one of several mathematical equations; therefore, the validity of free testosterone estimates are questionable. Calculated free testosterone should not be used to diagnose ‘low testosterone’ in women.
The adrenal glands also produce 11-oxyandrogens, which are 11-oxygenated androstenedione and testosterone.3 After entering the circulation, they are converted to 11-ketoandrogens (Figure). It has been shown that 11-ketotestosterone and 11-ketodihydrotestosterone activate the androgen receptor similar to testosterone and DHT. However, more studies are needed to establish whether these 11-oxyandrogens are biologically important with respect to physiology and pathophysiological conditions.3,4
What happens to androgens in the menstrual cycle and with ageing?
The variation in testosterone concentrations across the menstrual cycle parallel those of oestradiol, with a nadir in the menstrual phase followed by higher concentrations midcycle and during the luteal phase.4 There have been suggestions that testosterone levels may be higher in the morning, but a diurnal variation has not been seen in studies using liquid chromatography, tandem mass spectrometry (LC-MS/MS).5 In premenopausal women, circulating levels of all the androgens decline gradually with age.4 Thereafter, there is a steady reduction with ageing in DHEA and DHEAS levels. Whereas testosterone concentrations decline throughout the reproductive years, with a nadir observed in women in their early 60s, there is a small increase from their eighth decade of life, and these older women have similar testosterone levels as premenopausal women.6 Women who undergo bilateral oophorectomy before their natural menopause experience an approximate 50% drop in their circulating testosterone and androstenedione levels. Furthermore, women with primary ovarian insufficiency have significantly lower androgen levels compared with age-matched women with regular menstrual cycles.7 These conditions demonstrate the importance of the ovarian contribution to androgen levels in premenopausal women.
LC-MS/MS offers greater sensitivity and precision for the measurement of testosterone in women, and eliminates the problem of cross-reactivity between testosterone and other steroids encountered with standard immunoassays.4,8 Hence, median circulating testosterone concentrations in healthy young women measured by LC-MS/MS are lower than those measured by immunoassays.
As virtually all measurement of testosterone in the clinical setting in Australia is by immunoassay, which lacks precision at low concentrations in women, testosterone levels should not be measured to diagnose ‘testosterone insufficiency’ but rather to identify women who have unexpectedly high/high normal levels, suggesting the sexual issue is unlikely to improve with testosterone therapy.9 Testosterone levels should be measured in women treated with testosterone to monitor for overtreatment.9 Generally, a testosterone concentration of more than 50% above the upper limit of the standard/normal reference range of the laboratory used would be taken as excessive therapy requiring a lowering of the dose used.
Testosterone therapy for women
The care of women with sexual problems includes identification and modification of potential contributing factors, sexual and/or relationship counselling, education and, if indicated, a trial of testosterone therapy. It is important to determine early on in the assessment of a sexual problem if it has been lifelong or acquired, generalised or situational. Sexual counselling is the first step for women presenting with lifelong and/or situational dysfunction as these characteristics indicate strong underlying psychosocial and relationship issues. It is important to recognise that no cutoff blood level of any androgen measured can be used to differentiate women with sexual dysfunction from those without.9
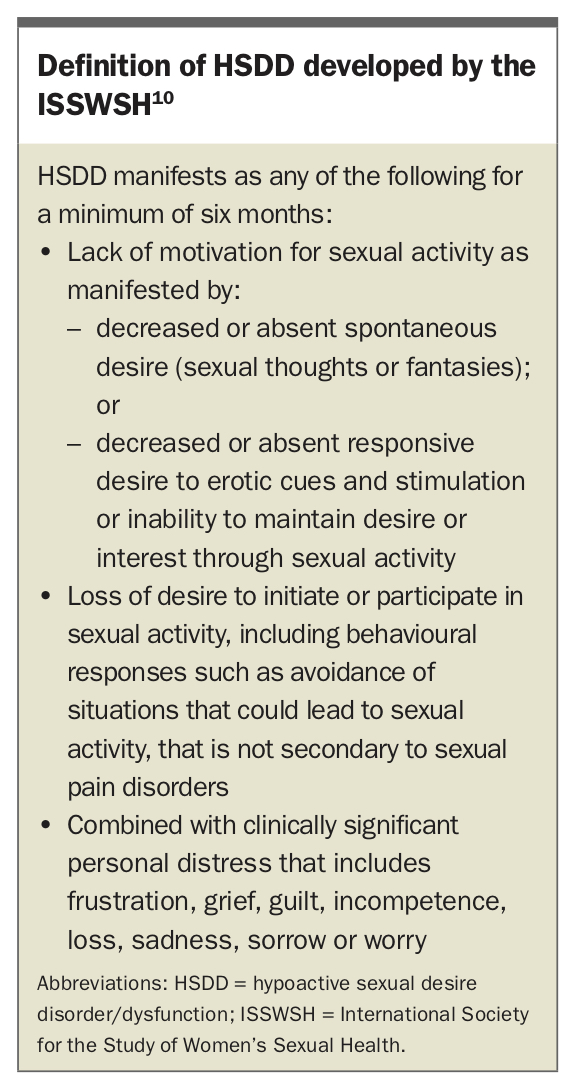
The first global consensus position statement on the use of testosterone therapy for women concluded that the only evidence-based indication for testosterone therapy is the treatment of low sexual desire that causes the affected woman personal distress (hypoactive sexual desire disorder/dysfunction; HSDD).9 Although in clinical practice androgen therapy for women mainly refers to testosterone use, other formulations marketed as androgen therapy include oral DHEA, which has not been shown to be effective for the treatment of sexual dysfunction in postmenopausal women and should not be used for this purpose.9 The diagnosis of HSDD in the clinical setting should be based on symptoms guided by diagnostic criteria such as those from the International Society for the Study of Women´s Sexual Health (ISSWSH; Box) or the International Classification of Diseases 11th Revision.10,11 The ISSWSH developed an open access process of care algorithm for the management of HSDD in women, useful for clinical practice.10
{kind=link}
Is it safe and effective?
A comprehensive systematic review and meta-analysis of published clinical trials of testosterone therapy for women reported clear beneficial effects of testosterone over placebo in postmenopausal women with HSDD, with or without concurrent estrogen treatment.12 Improvements were seen in the frequency of satisfying sexual events, sexual desire, arousal, orgasm and responsiveness, and self-image, as well as in the reduction of sexually-related distress. For all other outcomes evaluated, except wellbeing, the available data for analysis was too limited for the findings to be considered conclusive. There are sparse data available for premenopausal women such that the use of testosterone for HSDD or other outcomes in premenopausal women is not supported.12
Testosterone therapy should only be prescribed in doses that achieve physiological blood concentrations, as seen in premenopausal women, avoiding supraphysiological levels that could cause adverse effects.12 Therefore, to reach adequate systemic concentrations it is essential to use nonoral formulations, such as transdermal testosterone. Formulations such as compounded subcutaneous pellets, injectable testosterone and compounded ‘bioidentical’ testosterone lack evidence of efficacy and safety, and may expose women to the risk of virilisation due to supraphysiological testosterone concentrations. The 2019 global position statement recommends strongly against the use of compounded testosterone except in exceptional circumstances, which rarely apply in Australia and, if present, would require specialist referral.9
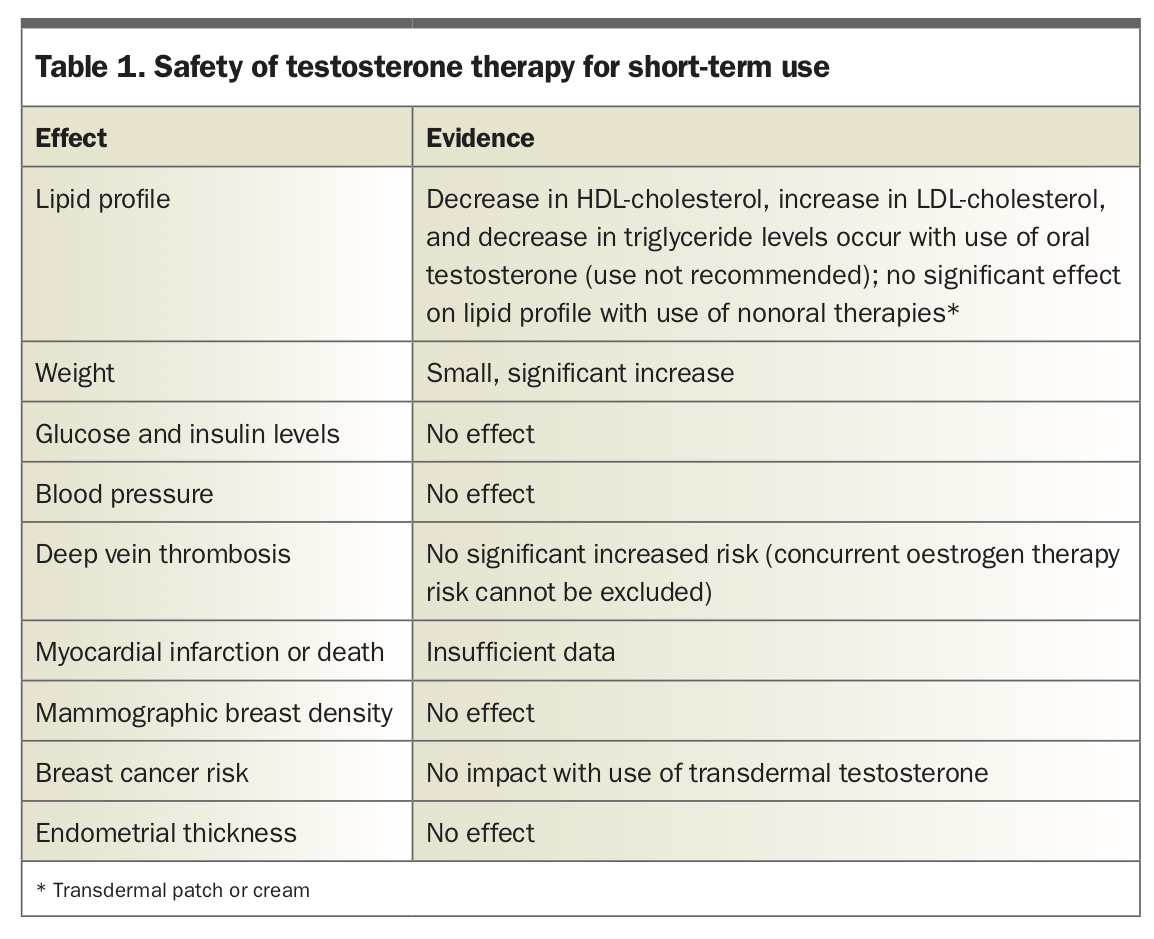
Side effects related to testosterone therapy, in clinical trials of postmenopausal women, have been limited to body/facial hair growth and acne in some women. Testosterone therapy, at doses approaching physiological levels in premenopausal women, has not been associated with serious adverse events. Women at high risk of cardiometabolic disease were excluded from randomised controlled trials of testosterone therapy; therefore, treatment recommendations cannot be generalised to those at-risk women. This also applies to breast cancer risk, as women with a breast cancer history were also excluded from clinical trials. Hence, caution is needed for women who have a history of hormone-sensitive breast cancer as testosterone can be converted to oestradiol in the breast. Such cases should be referred to a specialist. There have been claims that testosterone implants are associated with a reduced breast cancer risk, alone or combined with anastrozole pellets, but quality clinical trial data to support these claims are lacking.13 The safety concerns of testosterone therapy for short-term use (less than 24 months) are summarised in Table 1. The safety of testosterone therapy has not been established for long-term use.
{kind=link}
Prescribing and monitoring
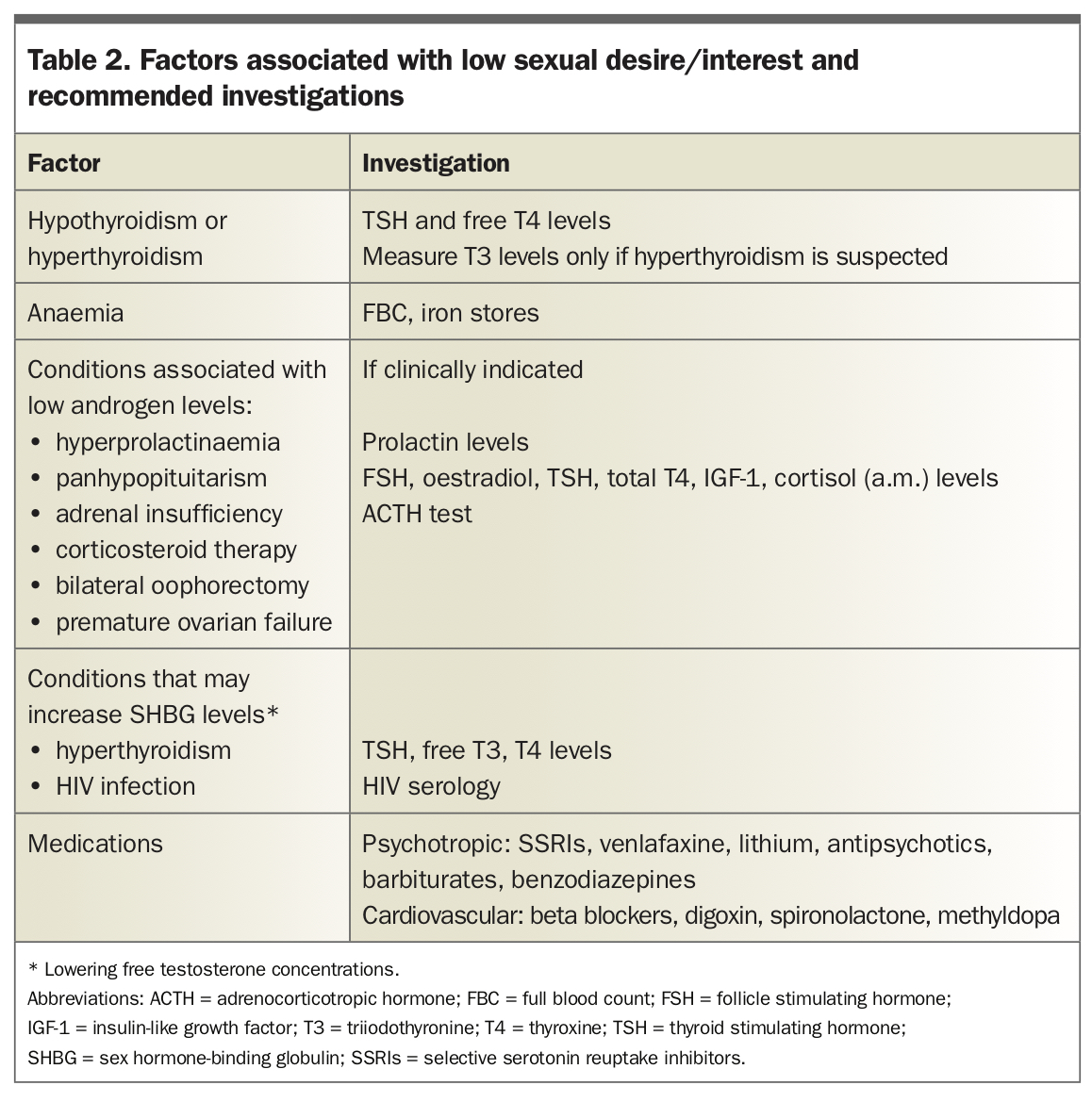
Testosterone therapy should be prescribed only after a full clinical assessment, including medical, sexual and social history, to identify potentially reversible factors. It is essential to ask about psychological, physical and sexual abuse, relationship issues, and knowledge and beliefs about sexuality. Physical examination is also important to identify any factor that may translate into low sexual desire (e.g. galactorrhoea related to hyperprolactinaemia, pale mucosa involving anaemia, untreated vulvovaginal atrophy causing dyspareunia and obviously low libido – excluding HSDD; Table 2).10
{kind=link}
Baseline total testosterone and SHBG levels should be measured before starting therapy, with repeat levels measured three to six weeks after treatment initiation. This will exclude women who have unexpectedly high levels from treatment. In Australia, a 1% transdermal testosterone cream, AndroFeme 1 (0.5 mL dose = 5 mg testosterone) is TGA approved for postmenopausal women with HSDD.14,15 This product is pharmacokinetically stable and has been shown to be effective in small studies in women with HSDD. It should be applied directly onto clean, dry skin of the upper outer thigh until absorbed. It should be explained that achieving an initial improvement in symptoms can take about four to eight weeks. Treatment should be discontinued if no improvement is experienced by the patient after six months of continuous therapy.9
Postmenopausal women taking oral estrogen hormone therapy with SHBG levels above the normal range have been found to be less responsive to testosterone therapy; switching to transdermal estrogen to reduce SHBG levels should be done before starting testosterone.
Alternatively, if a woman has a very low SHBG level, the testosterone dose needs to be reduced to avoid rapid clearance from the blood to the tissues and potential androgenic effects.
Evaluation of therapy includes clinical assessment of improvement in sexual function of testosterone and screening for signs of androgen excess, with testosterone and SHBG levels measured every six months to screen for inadvertent excess dosing.
Regulatory approved women’s formulations are urgently needed to address the necessity in most countries for women to be prescribed fractionated doses of male formulations, which expose women to side effects from supraphysiological dosing.
Conclusion
Testosterone levels gradually decline throughout women’s reproductive years, reaching a nadir in their 60s, with a small increase thereafter in older women to levels comparable with those seen in premenopausal women. Low sexual desire associated with distress or HSDD is not diagnosed by a low blood testosterone level. Instead, HSDD should be determined after a full clinical assessment, including medical, sexual and social history, to identify potentially reversible factors and other primary causes. When testosterone treatment is administered, blood levels should be monitored to avoid supraphysiological concentrations of the hormone. Moreover, regulatory approved women’s formulations of testosterone are urgently needed to ensure safety and enable research into long-term use. ET