Metabolic disease in mental illness: exercise as medicine

Exercise and physical fitness
Individuals living with mental illness have high rates of premature cardiometabolic disease. Reasons for this are complex but may include adverse effects of medications, such as antipsychotics, and poor access to physical health care. Incorporating regular physical activity as part of treatment for people with mental illness can help reduce cardiometabolic disease. General practitioners can play a key role in co-ordinating the appropriate services and referrals for such patients.
- People with mental illness have poorer health outcomes than the general population and are at higher risk of developing cardiometabolic disease, including diabetes, prediabetes, metabolic syndrome, obesity and premature cardiovascular diseases.
- Low levels of physical activity, adverse effects of atypical antipsychotic medications and factors, such as diet, health literacy and access to health care, affect physical health outcomes of people with mental illness.
- Increasing physical activity can benefit cardiometabolic outcomes and may improve symptoms of mental illness.
- The traditional separation of mental and physical health care and lack of referral pathways for people with mental illness should therefore be challenged across all healthcare settings.
- Individualised exercise programs for patients with mental illness, taking into account the patient’s motivation and preferred exercise and activity level, can help patients reach their exercise goals and maximise the benefits of physical activity.
- Some referral options to private and community-based exercise professionals and programs may be Medicare- rebatable and should be considered in the management of patients with mental illness who are at risk of metabolic disease.
An abundance of research indicates that physical health comorbidities, including premature cardiometabolic disease, are substantially more common across the spectrum of all mental illnesses compared with the general population.1-3 Significant progress in physical health care and an increasing life expectancy among the general population have not translated to those living with mental illness, who are at increased risk of premature cardiovascular morbidity and mortality.2-4 Diabetes, prediabetes, metabolic syndrome, obesity and premature cardiovascular diseases are twice as likely to occur in any person experiencing mental illness, contributing to a 15 to 30 year decrease in life expectancy. For those with psychotic disorders, 28.5 years of life may be lost.5-7 Although suicide contributes to mortality, 83% of premature mortality for this group is directly attributed to physical illness comorbidity.1,8
Factors contributing to poor physical health
Low levels of physical activity, adverse effects of atypical antipsychotic medications and other factors, such as diet, health literacy and access to health care, need to be considered in the prevention and management of the poor physical health outcomes of people with mental illness.
Antipsychotic medication
Although antipsychotic medications remain essential in the treatment of many people living with psychotic illness, they can contribute to physical morbidities and it is therefore important that physical health care is also addressed for these patients.9-11 Psychotropic medications can be a significant driver for weight gain, increased appetite, sedentary behaviour, central and visceral adiposity and elevated blood glucose levels.9-12 Patients may experience 10 to 15% or more increase in body weight over a 12-week period while on these medications.12
Hospitalisation
Hospitalised patients may experience 2 kg or more of weight gain per week during their admission, largely because of sedentary behaviour, increased eating patterns as a result of increased availability of food options, medication side effects, boredom and psychosocial stressors resulting from their hospital stay.13-15 This highlights the importance of exercise and dietary intervention for these populations.
Low levels of physical activity
The benefits of physical activity in mental illness have been well described, yet individuals living with severe mental illness engage in significantly higher levels of sedentary behaviour than the general population.1,16,17 This group is far less likely to meet the recommended 150 minutes of moderate physical activity per week.1,4,18 Physical health pathways for those with mental illness need to be established and accessible. General practitioners play an instrumental role in providing holistic care that includes provisions for physical activity.
Benefits of increased physical activity
Physical activity is beneficial in increasing insulin sensitivity, lean muscle mass, mitochondrial density, HDL cholesterol, cardiac output and glucose uptake, while reducing adipose tissue and central adiposity. Glucose is an important source of energy for skeletal muscles and exercise remains the most powerful stimulus for promoting the expression of the glucose transporter type 4 protein at the intracellular muscle sarcomere and T-tubules. This allows for greater glucose uptake, storage and metabolism by muscle cells.19-21 For people with mental illness, improving physical health alone can potentially translate to an estimated 46% reduction in the development of type 2 diabetes.22-24 Several meta-analyses indicate that exercise also improves the low-grade systemic inflammation characteristic of metabolic disease.19,25,26 In addition to the physical health benefits from improved inflammatory regulation, recent evidence suggests that physical activity also improves symptoms of schizophrenia, schizoaffective disorder, bipolar disorder and major depression.1,4,27
Recommendations for physical activity
A tailored approach to managing people with mental illness is needed for exercise programs to be effective. Exercise programs should be targeted and specific, and follow evidence-based practice to achieve mental health, physical health and patient–clinician goals.
How much physical activity is enough?
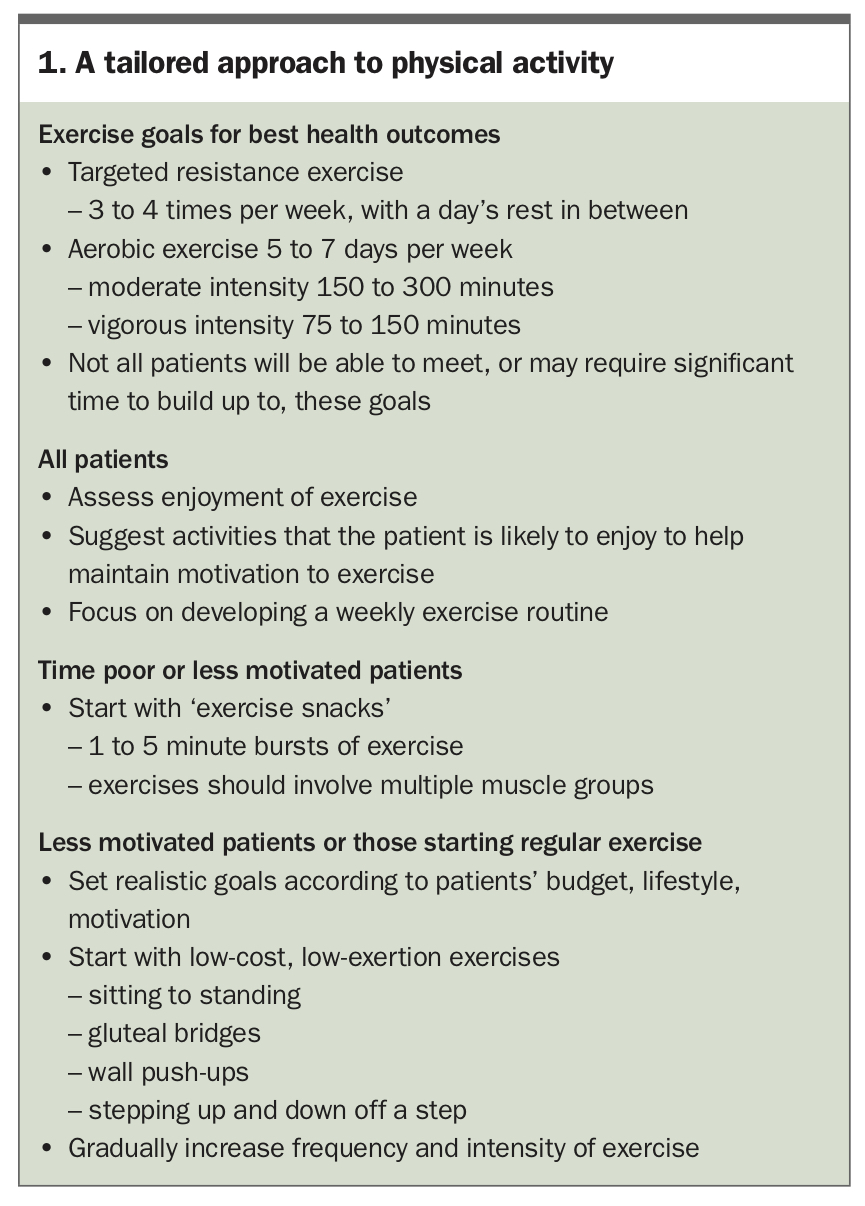
Targeted resistance exercise on three to four days per week, allowing for 24 hours of muscle rest between workouts, combined with aerobic exercise five to seven days per week at 150 to 300 minutes moderate intensity or 75 to 150 minutes vigorous intensity is an ideal general guide for best health and fitness outcomes (Box 1).28 However, these targets may be difficult to achieve for many, with less than 45% of adults in Australia meeting these physical activity guidelines.29 People with mental illness, who experience poorer physical health outcomes, may find it even more difficult to reach this goal.30
{kind=link}
Objective methods that measure intensity of exercise, such as heart-rate reserve target zones and rated perceived exertion scales, are not always practical or well understood. A practical approach to quickly determining exercise intensity is through a ‘talk test’: if you can talk but not sing during physical activity this is considered moderate intensity, but if you can neither sing nor talk due to exertion this is vigorous intensity.
How to approach the individual patient
Supervised exercise, which refers to structured exercise guided by an exercise professional, may remain the most effective method of reaching and maintaining long-term health benefits but may not be easily available.31-33 A patient’s motivation to exercise and their enjoyment of the exercise program is fundamental to their success in achieving their exercise goals, independent of access to supervised exercise.34-36 Starting or considerably changing an exercise program requires a strong focus on developing weekly routines. Encouraging patients to make small, incremental increases in their physical activity over time can help with habit forming and increase compliance to weekly routines. Personal enjoyment of exercise type and modality will vary and must be considered before gradually increasing frequency and intensity over time – particularly for patients with low motivation to exercise.34-36 A combination of home-based and supervised exercise programs are often used where limitations such as cost or poor access to community-based exercise programs persist.33
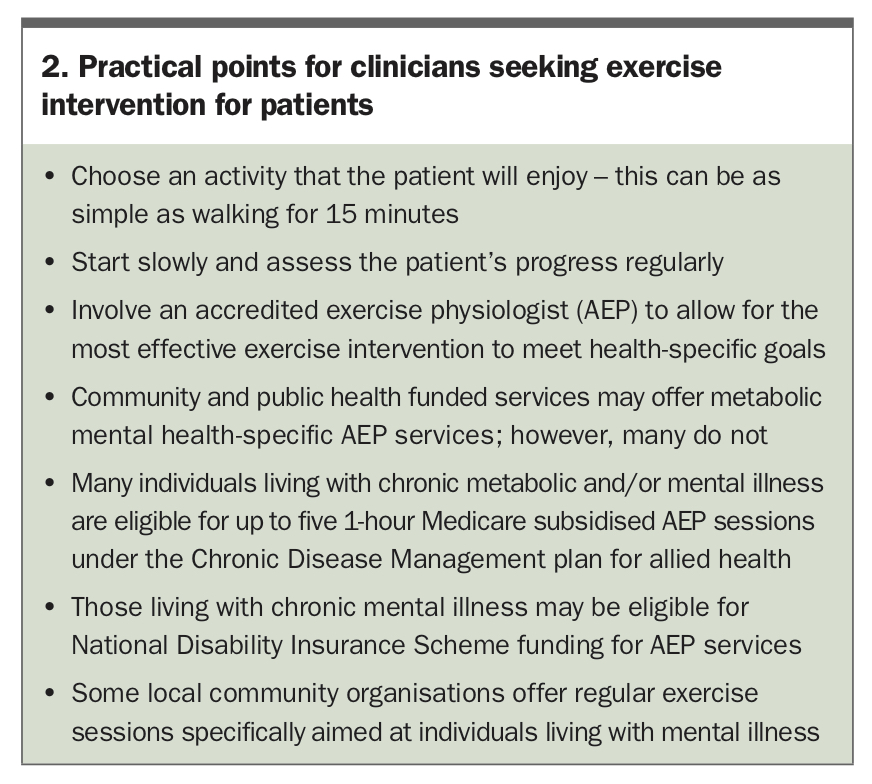
GPs and other clinicians are well placed to initially suggest exercise options such as walking programs or online workouts. ‘Exercise snacks’, whereby simple exercises involving multiple muscle groups are performed over a 1- to 5-minute period, are becoming increasingly popular, particularly for those who may be too busy or who are not motivated to engage in regular exercise. Low-cost, low-exertion exercises, such as sitting to standing, glute bridges, wall push-ups or stepping up and down off a step, may also be considered for patients with low motivation or those starting regular physical activity. Setting realistic goals suitable to a person’s budget and motivation to exercise is particularly important for those living with serious mental illness, as they may take a considerable amount of time to reach the recommended minimum of 150 minutes per week of moderate intensity exercise (Box 1). Approaches and pathways to help patients access the associated health benefits of increased physical activity are summarised in Box 2.
{kind=link}
Referral to an accredited exercise physiologist
Where available, the patient can be referred to an accredited exercise physiologist. An accredited exercise physiologist will combine trained behaviour change strategies, pathophysiological responses and gold standard health approaches across physical and mental illnesses and their related comorbidities to best meet clinician–patient goals safely. This intervention is likely to be cost-effective for health systems and patients alike. Accredited exercise physiologist interventions provide a high return on investment in treating people with chronic conditions, notably prediabetes and type 2 diabetes, mental illness (including physical comorbidities) and cardiovascular disease.37
How to refer a patient
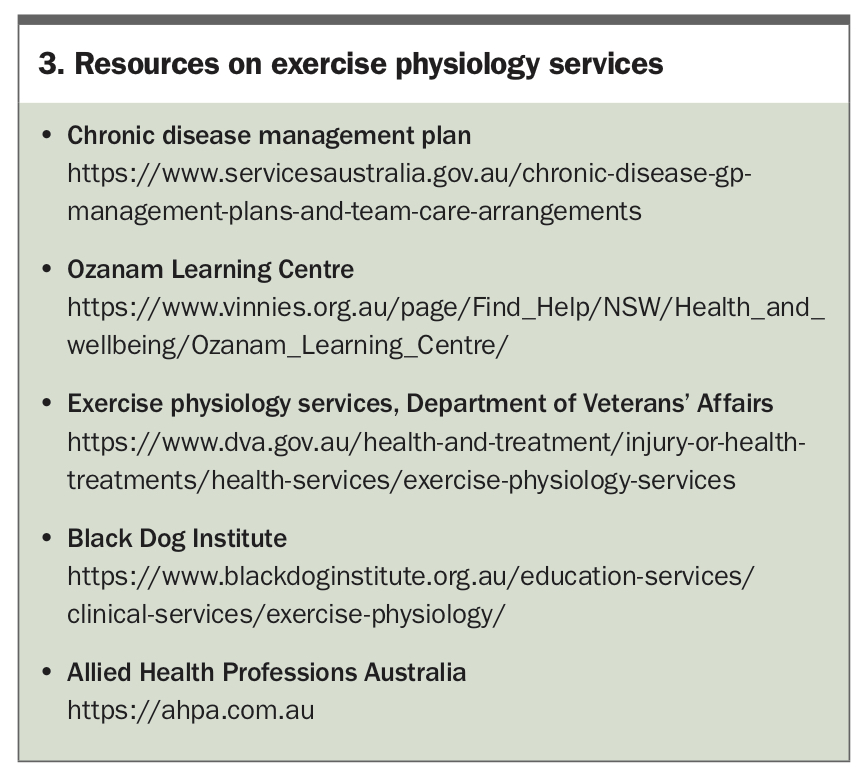
Patients who use community and public mental health services can be referred to exercise physiology services within those facilities if available, although availability remains sporadic. Where established accredited exercise physiology services are not available, patients can also be referred to an accredited exercise physiologist in private practice. These referrals may fall under the eligibility criteria for subsidised services via Medicare rebates under the national Chronic Disease Management plan for five one-hour sessions. Some people living with mental illness may be eligible for National Disability Insurance Scheme-funded services, which include exercise physiology. Some organisations within local communities also offer exercise physiology services at reduced rates, specifically targeted to those living with mental illness. These programs are usually state-based or run by non-government organisations working at the local level to create opportunities for people living with vulnerabilities (Box 3).
{kind=link}
Conclusion
Separation of physical and mental health services is still common. Referral pathways to metabolic services may not be available in most healthcare settings despite an abundance of research showing cost-effectiveness from service provision, positive clinical outcomes and increased advocacy. The GP can be central in providing and co-ordinating services. In the community, appropriate referral to an accredited exercise physiologist by GPs through care plans such as the Chronic Disease Management plan for Medicare subsidised sessions should be considered as part of a comprehensive treatment plan. If a patient does not regularly see a GP, care managers and community mental health workers are vital in providing treatment expertise and in recognising the value of initiating appropriate referrals for a treatment plan that incorporates physical health outcomes. ET