Jack is a 62-year-old man who presents to your rural general practice with a two-day history of headache, nausea and vomiting. In the past 24 hours he has become profoundly fatigued and is now finding it difficult to perform activities of daily living.
His significant past history is a melanoma resected from his back 10 years ago, with metastatic disease to the lungs, abdominal lymph nodes and liver diagnosed four months ago. He is seeing his oncologist in the city every three weeks for treatment, which commenced about two months ago. He has been tolerating treatment well, except for vitiligo of the skin and a pruritic rash, which he developed after the first treatment. He also experiences fatigue after each treatment cycle, which lasts for at least three days. His last treatment was one week ago. Other past medical illnesses include Hashimoto’s thyroiditis diagnosed 10 years ago, and hypertension. He is currently on irbesartan (his only medication).
What are your main concerns for Jack?
Answer: Jack’s symptoms are nonspecific and could represent his infusion reaction, although it is lasting longer than the usual course. It is important to exclude progression of Jack’s disease or an adverse effect related to his treatment. In the first instance, clarifying the location of the metastases and the nature of treatment is important.
A review of Jack’s medical record reveals that he has stage IV metastatic melanoma with lesions in his lung (bilateral, including mediastinal lymph node), liver and para-aortic lymph node. A lung nodule was biopsied before treatment started, which confirmed the diagnosis. Fluorodeoxyglucose PET scan and MRI brain were performed about three months ago (before the start of treatment) and excluded cerebral metastases. He is due for further imaging in one month’s time. He has been on combination ipilimumab and pembrolizumab for the past two months. The main adverse effects noted are the skin changes.
Advertisement
Does this refine your diagnosis?
Answer: It is reassuring that there are no known cerebral metastases, given his headaches, nausea and vomiting. The known abdominal lymph nodes could give the picture of gastrointestinal discomfort. Given that he has not had imaging done for three months there could be progression of his disease during this time. However, it is more likely he is experiencing a novel adverse effect to treatment.
How do ipilimumab and pembrolizumab work?
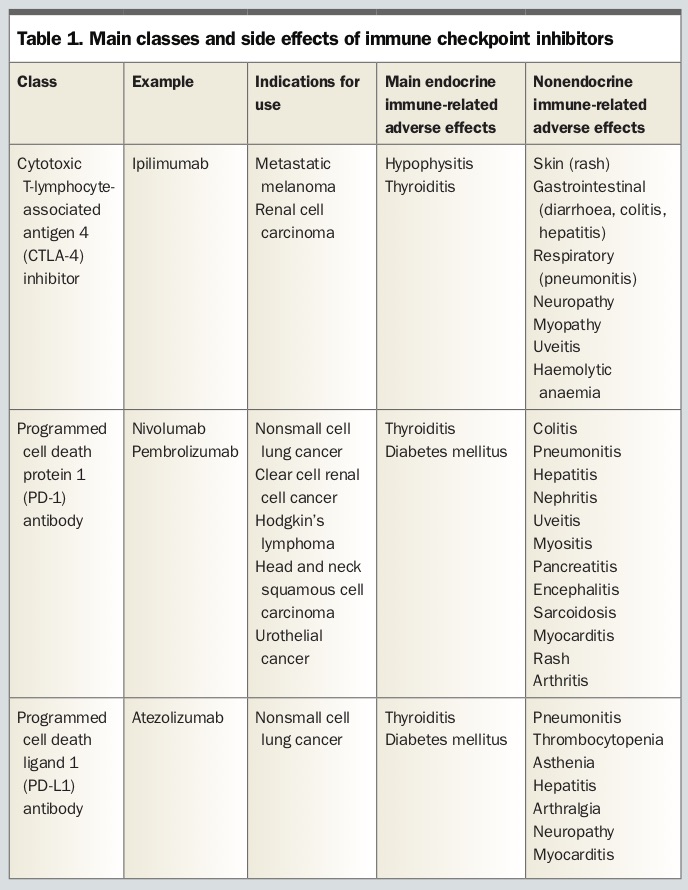
Answer: Ipilimumab is a cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitor, available on the PBS for the treatment of metastatic melanoma and renal cell carcinoma.
1,2 It is the only drug available for use in this class. Pembrolizumab is a programmed cell death protein 1 (PD-1) antibody, available on the PBS for the treatment of melanoma, nonsmall cell lung cancer, and head and neck squamous cell carcinoma.
3 Nivolumab is a PD-1 inhibitor additionally approved for use in clear cell renal cancer, Hodgkin’s lymphoma and urothelial carcinoma.
4 There are also PD ligand 1 (PD-L1)inhibitors (e.g. atezolizumab). Together these drugs are a novel class of cancer treatment known as immune checkpoint inhibitors (ICIs) (
Table 1).
ICIs aim to manipulate the immune system to offer a novel target for susceptible cancer types. Both CTLA-4 and PD-1 are involved in protection against T-cell mediated self-antigen destruction. CTLA-4 inhibitors block T-cell inhibition, which leads to T-cell potentiation. PD-1 is expressed on T-cells and PD ligand on tumour cells. The interaction between these prevents the tumour cells from being destroyed by inflammatory cells. PD-1 and PD-L1 inhibitors disrupt this negative signal and allow tumour cells to be susceptible to destruction.
These drugs were first used to treat melanoma, improving overall survival and progression of disease, with greater efficacy in combination therapy than monotherapy of either class.
What are the side effects?
Answer: As a result of their unique mode of action (different to traditional cytotoxic chemotherapy) there are new immune-related adverse effects (irAEs) of ICIs.5-7 The spectrum depends on the ICI given, with more irAEs in combination therapy than monotherapy, the dose of the ICI and the tumour type being treated. In melanoma, the most common irAEs are seen in the skin, including vitiligo and rash (occurring in more than 30% of patients), and gastrointestinal (occurring in about 15% of patients). These have a median time of onset of less than eight weeks. Other irAEs include hepatic dysfunction (median time to onset seven weeks), respiratory (nine weeks) and endocrine dysfunction (10 weeks). It should be noted that irAEs can occur many months after initiation of therapy and even after therapy has been suspended.8
Advertisement
What are the endocrine immune-related adverse effects?
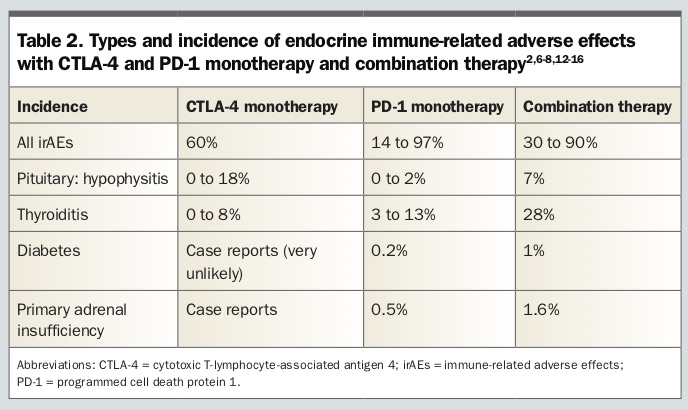
Answer: Endocrine irAEs primarily involve the pituitary, thyroid and, rarely, the adrenal glands and pancreas.
8 Table 2 details the incidence of the most common endocrine irAEs. Pituitary involvement usually manifests as hypophysitis, resulting in the loss of one or more of the pituitary hormones, including adrenocorticotrophic hormone (ACTH), thyroid stimulating hormone (TSH), luteinising hormone (LH) and follicle stimulating hormone (FSH) resulting in hypoadrenalism, hypothyroidism and/or hypogonadism. These patients rarely develop posterior pituitary dysfunction in the form of diabetes insipidus, unless there has been structural damage due to cerebral lesions, surgery or radiotherapy.
The thyroid can become overactive or underactive, and is almost exclusively due to thyroiditis or inflammation of the thyroid gland rather than over-production. However, patients who have previously had Graves’ disease can develop flares, as is common for many other previously diagnosed autoimmune conditions. Thyroiditis can manifest as hyperthyroidism followed by euthyroidism or hypothyroidism, or primary hypothyroidism. Once a patient has commenced on thyroxine they are rarely able to come off the medication, that is, once gland failure has occurred it is usually permanent.
Pancreatic endocrine dysfunction manifesting as diabetes can also occur resulting in ketoacidosis. Patients present in a similar way to patients with type 1 diabetes and often require lifelong insulin therapy. Primary adrenal failure is rare and reported in cases only.
In what way could Jack’s presentation be a manifestation of endocrine irAEs?
Answer: The symptoms of headache, nausea and vomiting could represent hypophysitis. Further examination to suggest this includes a postural drop in blood pressure. Urgent investigation is important to exclude this irAE.
What investigations would you perform to clarify the diagnosis?
Answer: The best investigations to perform are a cortisol measurement in the early morning with a matched ACTH. However, given the urgency of the presentation a cortisol measurement taken at any time is helpful. Review of the imaging of the brain is also helpful, and repeat imaging is sometimes required to exclude metastatic disease. Hypophysitis can sometimes be seen on MRI with a swollen pituitary gland and thickened pituitary stalk, but these radiological changes often improve after treatment.
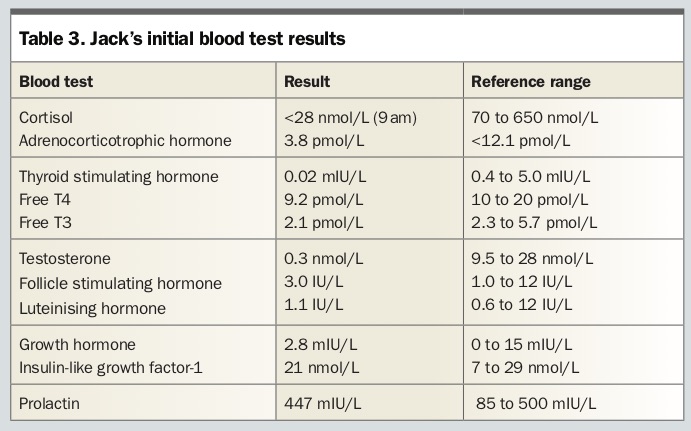
If the cortisol level is abnormal, completion of the pituitary screen including TSH, free T4, electrolytes, prolactin, testosterone, LH and FSH may give clues on the diagnosis and deficiencies of other hormones.
Jack’s blood test results are shown in Table 3, with the main abnormality being the low cortisol level. The T4 level is low with an inappropriately normal TSH level suggesting central or secondary hypothyroidism. Testosterone is also low with inappropriately normal FSH and LH levels suggesting secondary hypogonadism.
Advertisement
How would you interpret the cortisol level?
Answer: In a patient who has been on ICIs, particularly with CTLA-4 monotherapy or combination therapy, the diagnosis of hypophysitis should be strongly suspected, especially with the presence of symptoms.
Other diagnoses to consider include physiological low cortisol levels in the afternoon and overnight, use of exogenous steroids and adrenal disease. Cortisol release has a circadian rhythm, with highest levels in the pre-dawn time and lowest at midnight. Sampling in the afternoon and evening will yield a lower result. It is also important to bear in mind cortisol levels at different laboratories may have different reference ranges depending on the methods used.
Exogenous steroids are commonly used for patients with malignancy, including dexamethasone, which would cause a low cortisol level due to suppression of the hypothalamic-pituitary-adrenal axis. It is also important to exclude the use of inhaled corticosteroids and topical glucocorticoids (including eye drops) as causes of falsely low cortisol levels, although these medications do not universally cause completely suppressed cortisol levels.
Adrenal diseases can include bilateral adrenal haemorrhage, bilateral metastases or ICI-related hypoadrenalism, although this has rarely been reported. Adrenal disease causing hypoadrenalism would be associated with an elevated ACTH level, which is not present in Jack’s case.
How does hypophysitis present?
Answer: Patients often have nonspecific symptoms including headache, nausea, vomiting and abdominal pain. Onset is rapid, and patients can become unwell within days. Rarely do patients develop any neurological deficits (due likely to the rapidity of the inflammation of the pituitary). Hence patients would not often have visual field deficits, diplopia or decreased visual acuity.
How will you manage Jack?
Answer: Once the diagnosis is suspected, the most important hormone to replace is glucocorticoids. The initial dose depends on the clinical state of the patient. Patients who are haemodynamically unstable require urgent parenteral glucocorticoids, hydrocortisone 50 to 100 mg three times daily. High-dose corticosteroids do not appear to prevent the progression of hypophysitis to long-term hormonal replacement.9 Those who can tolerate oral intake and are stable but unwell (as Jack is) should have an oral stress dose of equivalent prednisone 25 to 50 mg daily. This dose can be gradually weaned over the ensuing two to three weeks depending on the clinical presentation. Earlier recognition of presentations of hypophysitis often prevents hospitalisation and management in the outpatient setting. However, if there is any doubt on the severity of Jack’s symptoms, it is important to involve his treating oncology team and local hospital emergency department.
Advertisement
Long-term maintenance dose titration depends on the patient’s blood pressure and energy levels, and is usually the equivalent of 2.5 to 5.0 mg prednisone daily.10 Hydrocortisone (10 to 20 mg daily) or cortisone acetate (12.5 to 25 mg daily) can also be used and is particularly useful in patients requiring split dosing, or varying dosing during the day. In addition, hydrocortisone and cortisone have the advantage of less long-term effects on bone mineral density but require careful titration to the lowest required dose. Hydrocortisone and cortisone should be given in two to three split doses during the day. Doses should be uptitrated, taking into account the patient’s symptoms and weight. However, there is a lack of evidence on the optimal regimen to provide a patient, balancing improving clinical symptoms with prevention of side effects of over-replacement.11
It is important to discuss stress management of glucocorticoids with patients, particularly those with infective illnesses, gastrointestinal illness where oral glucocorticoids may not be easily absorbed, and elective surgery where patients have fasted. Most patients who have developed hypophysitis do not recover pituitary function and require long-term hormone replacement.
Jack also likely requires thyroxine replacement given his low free T4, free T3 and inappropriately low TSH levels. It is important to replace this after glucocorticoids, as unopposed thyroxine replacement in patients with hypophysitis can lead to adrenal crisis due to increased basal metabolic rate and increased cortisol clearance. The dose of thyroxine would be about 1.6 mcg/kg daily (i.e. a full replacement dose is required).
Testosterone replacement may be required, but low levels can sometimes be a stress response and recover to normal levels in several months time.
How should Jack be followed up in the long term?
Answer: It is important to assess Jack’s glucocorticoid replacement and ensure the dose is adequate. The importance of stress dosing should be reiterated and intramuscular injection of hydrocortisone should be prescribed with an appropriate family member taught how to administer this.
Even if patients do not develop hypothyroidism at onset they may lose other axes later, so it is important, particularly with ACTH and TSH, to monitor these regularly later on.
What is the prognosis of endocrine irAEs?
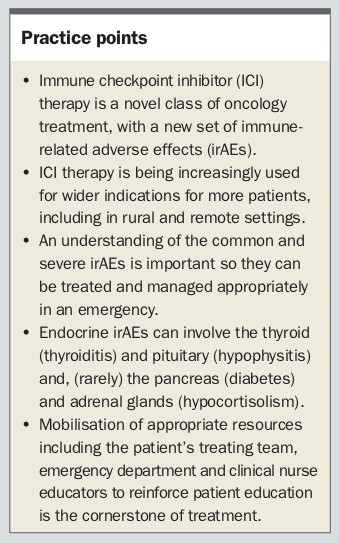
Answer: There are currently no reliable markers to predict the onset of endocrine irAEs and the presentation of hypophysitis is often rapid. It is important to note that once a gland fails due to ICIs it does not recover, and patients are on lifelong glucocorticoid, thyroxine or gonadal replacement. However, most patients only have mild grade 1 and 2 symptoms and many can be appropriately managed in the outpatient setting. (See
Practice Points box for handy tips.)
COMPETING INTERESTS: None.
Advertisement
References
1. Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Am J Clin Oncol 2016; 39: 98-106.
2. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010; 363: 711-723.
3. Robert C, Schachter J, Long GV, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med 2015; 372: 2521-2532.
4. Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med 2015; 372: 320-330.
5. Champiat S, Lambotte O, Barreau E, et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol 2016; 27: 559-574.
6. Weber JS, Hodi FS, Wolchok JD, et al. Safety profile of nivolumab monotherapy: a pooled analysis of patients with advanced melanoma. J Clin Oncol 2017; 35: 785-792.
7. Sznol M, Postow MA, Davies MJ, et al. Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treat Rev 2017; 58: 70-76.
8. Scott ES, Long GV, Guminski A, Clifton-Bligh RJ, Menzies AM, Tsang VH. The spectrum, incidence, kinetics and management of endocrinopathies with immune checkpoint inhibitors for metastatic melanoma. Eur J Endocrinol 2018; 178: 175-182.
9. Horvat TZ, Adel NG, Dang TO, et al. Immune-related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering Cancer Center. J Clin Oncol 2015; 33: 3193-3198.
10. Debono M, Ross RJ. What is the best approach to tailoring hydrocortisone dose to meet patient needs in 2012? Clin Endocrinol 2013; 78: 659-664.
11. Murray RD, Ekman B, Uddin S, Marelli C, Quinkler M, Zelissen PM. Management of glucocorticoid replacement in adrenal insufficiency shows notable heterogeneity - data from the EU-AIR. Clin Endocrinol 2017; 86: 340-346.
12. Ryder M, Callahan M, Postow MA, Wolchok J, Fagin JA. Endocrine-related adverse events following ipilimumab in patients with advanced melanoma: a comprehensive retrospective review from a single institution. Endocr Relat Cancer 2014; 21: 371-381.
13. Corsello SM, Barnabei A, Marchetti P, De Vecchis L, Salvatori R, Torino F. Endocrine side effects induced by immune checkpoint inhibitors. J Clin Endocrinol Metab 2013; 98: 1361-1375.
14. Min L, Hodi FS, Giobbie-Hurder A, et al. Systemic high-dose corticosteroid treatment does not improve the outcome of ipilimumab-related hypophysitis: a retrospective cohort study. Clin Cancer Res 2015; 21: 749-755.
15. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med 2017; 377: 1345-1356.
16. Gonzalez-Rodriguez E, Rodriguez-Abreu D. Immune checkpoint inhibitors: review and management of endocrine adverse events. Oncologist 2016; 21: 804-816.


{kind=link}
{kind=link}
{kind=link}
{kind=link}