The World Health Organization (WHO) refers to ‘hyperglycaemia first detected in pregnancy’ with subdivision into ‘diabetes mellitus in pregnancy’ and ‘gestational diabetes mellitus (GDM)’ (Figure).1 Although most women with hyperglycaemia first detected in pregnancy have GDM, some women have glucose levels in the range for diabetes outside pregnancy, which indicates possible undiagnosed diabetes (usually type 2 diabetes, occasionally type 1 diabetes). It is particularly important to identify women with diabetes mellitus in pregnancy because the management, especially obstetric, differs from that of GDM. Not all women with diabetes mellitus in pregnancy will continue to have diabetes when retested postpartum.
Hyperglycaemia in pregnancy now affects 10 to 30% of all pregnancies in Australia. The increasing prevalence has been driven by changes to the diagnostic process and criteria, on the background of an increasingly older, more obese, ethnically diverse pregnant population. Over the past 10 years, the diagnostic criteria have been heavily debated by the medical and obstetric community, a debate that has dominated the field. However, among the ‘noise’ of the debate, it is important for clinicians to have a sound, practical understanding of who, when and how to test for hyperglycaemia in pregnancy, as well as the main principles of management during pregnancy and postpartum.
To make this review as clinically relevant as possible, a case study is presented and several issues surrounding the diagnosis and management are discussed.
Case scenario
Lucy is a 42-year-old Caucasian woman who is six weeks pregnant in her second pregnancy. She has made an appointment to see you, her GP, for antenatal advice. Lucy was diagnosed with GDM in her first pregnancy two years ago at 26 weeks’ gestation and was treated with dietary adjustments. She delivered a healthy girl, weighing 3600 g at 39 weeks’ gestation via normal vaginal delivery. There were no neonatal complications. Lucy underwent a postpartum oral glucose tolerance test (OGTT) and reports that the result was normal. Lucy is otherwise well and does not have any other significant medical issues. She has a family history of diabetes. Her 62-year-old father was diagnosed with type 2 diabetes five years ago and is treated with metformin and Lucy’s sister had GDM that was treated with insulin. Lucy does not take any regular medication, but started taking a pregnancy multivitamin last week. On examination today, Lucy’s blood pressure is 100/70 mmHg. Her body mass index (BMI) is 27 kg/m2 (weight 72 kg, height 1.63 m).
Advertisement
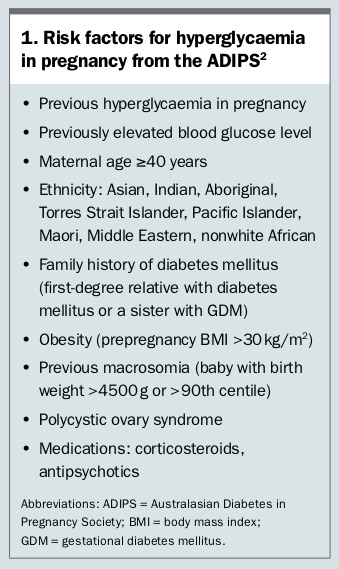
What are Lucy’s risk factors for hyperglycaemia in pregnancy?
Lucy’s risk factors for hyperglycaemia in pregnancy include previous GDM and a family history of diabetes (first-degree-relative with diabetes and a sister with GDM). A summary of risk factors for hyperglycaemia in pregnancy, as outlined by the Australasian Diabetes in Pregnancy Society (ADIPS), is summarised in
Box 1.
2
What are the potential adverse consequences of hyperglycaemia in pregnancy for Lucy and her baby?
Hyperglycaemia in pregnancy is associated with an increased risk of adverse maternal and neonatal outcomes. For Lucy, there is an increased risk of gestational hypertension, pre-eclampsia and obstetric intervention, as well as a 50% lifetime risk of developing diabetes, usually type 2 diabetes. For Lucy’s baby, there is an increased risk of macrosomia, stillbirth, birth trauma and metabolic complications such as neonatal hypoglycaemia and respiratory distress syndrome. In recent years, more evidence has emerged regarding the deleterious link between maternal hyperglycaemia in utero and an increased future risk of diabetes and obesity in the offspring, mediated by epigenetic changes in developmentally important genes in utero.3,4
Diabetes and obesity in the offspring can occur as early as childhood, particularly in very high-risk ethnic groups. Thus, in addition to genetic and environmental risk factors for diabetes, exposure to maternal hyperglycaemia in utero may amplify the ‘vicious cycle’ of diabetes and obesity from one generation to the next.
What is the relevance of the postpartum OGTT following Lucy’s first pregnancy?
If the postpartum OGTT from Lucy’s first pregnancy was consistent with diabetes or prediabetes, Lucy should be immediately referred to a specialist diabetes service for management. If the postpartum OGTT was normal, Lucy should be screened for hyperglycaemia in pregnancy in this pregnancy.
You locate Lucy’s postpartum OGTT -result from after her first pregnancy. The result was normal.
Should you arrange glucose testing for Lucy now or wait and test for GDM at
24 to 28 weeks’ gestation?
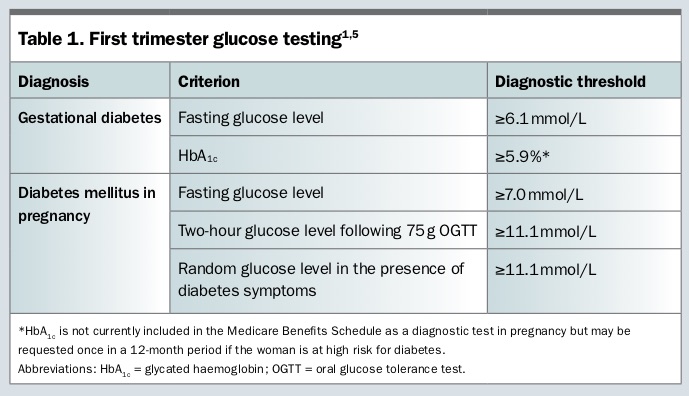
Lucy has risk factors for hyperglycaemia in pregnancy and should be tested in early pregnancy. The main aim of testing in early pregnancy is to identify women with undiagnosed type 1 or type 2 diabetes. The approach to glucose testing in early pregnancy is controversial. ADIPS recommends that the method of early pregnancy testing should be based on ‘clinical judgment, local healthcare policy and possible risk stratification,’ but should ideally be an OGTT or glycated haemoglobin (HbA
1c).
2 The WHO defines ‘diabetes mellitus in pregnancy’ as a fasting glucose level of 7.0 mmol/L or above and/or a two-hour glucose level of 11.1 mmol/L or above following a 75 g OGTT, or a random glucose level of 11.1 mmol/L or above in the presence of diabetes symptoms (
Table 1).
1 These thresholds are the same as those used to diagnose diabetes outside pregnancy. The 2018 Commonwealth Pregnancy Care Guidelines support the use of HbA
1c or fasting blood glucose in the first trimester, ideally at the first antenatal visit.
5 These guidelines recommend an HbA
1c level of 5.9% or above or a fasting glucose level of 6.1 mmol/L or above to diagnose hypergly-caemia in early pregnancy (
Table 1).
5 The fasting glucose threshold of 6.1 mmol/L is the same as that used to diagnose impaired fasting glucose outside pregnancy. HbA
1c is not currently included in the Medicare Benefits Schedule as a diagnostic test in pregnancy but may be requested once in a 12-month period if the woman is at high risk for diabetes.
Advertisement
Lucy’s fasting glucose level at seven weeks’ gestation is 5.0 mmol/L, which is normal.
What is your advice to Lucy regarding weight gain during pregnancy?
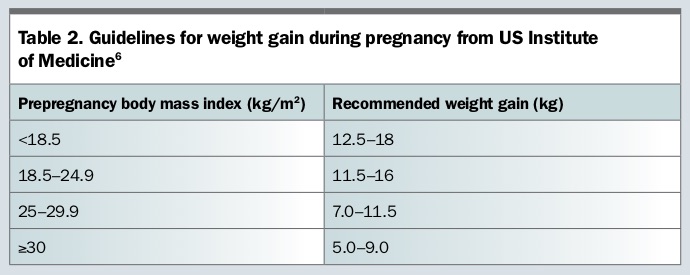
Lucy’s prepregnancy BMI is in the overweight category. A BMI in the overweight range increases Lucy’s risk of pregnancy complications, such as congenital anomalies, stillbirth, preterm birth, low birthweight, a large-for-gestational-age baby, gestational hypertension, pre-eclampsia, postpartum haemorrhage and major depressive disorders.
5 The US Institute of Medicine (IOM) developed guidelines for weight gain during pregnancy, based on prepregnancy BMI (
Table 2).
6 Recent Australian data support the use of the IOM guidelines in women with GDM.
7 However, at the time of GDM diagnosis, one-third of overweight women and half of obese women have already exceeded the IOM target intended for the entire pregnancy.
8 Therefore, it is important to educate Lucy in early pregnancy regarding appropriate weight gain during pregnancy.
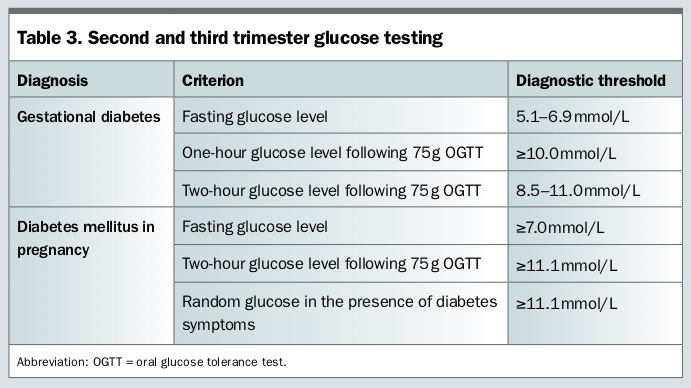
Should Lucy be tested for GDM at 24 to 28 weeks’ gestation?
Yes, even though Lucy does not have hyperglycaemia in early pregnancy, she may develop GDM later in pregnancy. Insulin resistance increases as pregnancy progresses, so a normal result in early pregnancy does not preclude the development of GDM later in the pregnancy. The thresholds for GDM in later pregnancy differ from those in early pregnancy (
Table 3).
Lucy is now 27 weeks pregnant and had a repeat 75 g two-hour OGTT at 26 weeks’ gestation. Her results are 5.6 mmol/L, 9.8 mmol/L and 8.6 mmol/L for fasting, one-hour and two-hour glucose levels, respectively, which are diagnostic for GDM. You refer Lucy to a specialist diabetes service for management.
What is the general management approach for GDM?
The main components of GDM management include patient education, self-monitoring of blood glucose, dietary advice, physical activity and, potentially, use of insulin. If possible, a multidisciplinary team, including a diabetes educator and dietitian, should be involved. Self-monitoring of blood glucose is usually performed four times daily, including fasting and one-hour or two-hour postprandial testing. Dietary advice focuses on evenly distributing carbohydrates, preferably those of a lower glycaemic index, across three main meals, interspersed with three snacks, to minimise postprandial glucose excursions, while meeting the nutritional requirements of pregnancy. Low-to-moderate-intensity physical activity is associated with a range of health benefits in pregnancy and can also minimise post-prandial glucose excursions, particularly if undertaken soon after meals.
Medical therapy, usually insulin, is indicated if self-monitoring of blood glucose testing demonstrates persistently elevated glucose levels despite appropriate diet and physical activity. Usually, an intermediate-acting insulin is given before bedtime to target elevated -fasting glucose levels. A rapid-acting insulin analogue, such as insulin aspart or insulin lispro, is given immediately before meals to target elevated postprandial glucose levels. Metformin is an option although is not universally recommended in women with GDM because of ongoing concerns regarding potential long-term effects from placental transfer of metformin to the fetus. Also, metformin is less effective in controlling fasting hyperglycaemia.
Advertisement
Obstetric monitoring is usually increased in women with GDM. Serial ultrasounds from about 28 weeks’ gestation are useful for monitoring fetal growth, although there is no consensus on the frequency. The timing and mode of delivery are determined by the obstetric team, taking into account maternal and fetal well-being, fetal size and potential risks including stillbirth, operative intervention and birth trauma. Most women will give birth between 38 and 40 weeks’ gestation. The aim is vaginal delivery unless there are obstetric indications for caesarean. Intensive glucose monitoring is required during labour. Supplemental subcutaneous insulin or an insulin-dextrose infusion may occasionally be required to optimise glucose levels and reduce the risk of neonatal hypoglycaemia. The route of insulin administration during labour depends on local policy.
Postpartum, any insulin therapy is ceased and the mother should be encouraged to breastfeed and continue a healthy diet. The infant is monitored for hypoglycaemia, signs of respiratory distress and other metabolic complications. Early postpartum self-monitoring of blood glucose is usually performed for one day (fasting and two hours after each meal) in the first four days postpartum. Most women do not need to continue self-monitoring of blood glucose levels unless there are concerns that diabetes or prediabetes might be present, which is more likely for women with diabetes mellitus in pregnancy than for those with GDM.
Lucy sees the diabetes educator and dietitian, but after two weeks of dietary management she is commenced on four insulin injections daily until she is induced at 39 weeks’ gestation. Lucy gives birth to a healthy baby girl, weighing 3850 g, with no neonatal complications. Her early postpartum self-monitoring of blood glucose levels in hospital were normal. She sees you at two months postpartum for a routine postnatal review.
Should you repeat the OGTT postpartum?
Yes, even though Lucy’s early postpartum self-monitoring of blood glucose levels was normal, it is not a diagnostic test for diabetes. Lucy should have a 75 g two-hour OGTT at six to 12 weeks postpartum to check for persisting abnormal glucose tolerance (pre-diabetes or diabetes). Women with evidence of prediabetes or who are planning another pregnancy should have an OGTT every one to two years; otherwise an OGTT or HbA1c every two to three years should suffice.
How can Lucy reduce her risk of hyperglycaemia in future pregnancies?
Lucy has a 30 to 80% risk of developing hyperglycaemia in a future pregnancy and a 50% risk of developing future diabetes.
9,10 The degree of these risks is modifiable, so Lucy should be encouraged to maintain a healthy lifestyle, with a balanced diet and regular exercise. BMI is a modifiable risk factor for future hyperglycaemia in pregnancy. One study demonstrated that, for women with GDM and prepregnancy overweight or obesity, a reduction in BMI by 2.0 kg/m
2 or more between pregnancies reduced the risk of subsequent GDM by 74%.
11 If Lucy reduces her prepregnancy weight by 6 kg to 66 kg, her BMI will fall from 27 to 24.8 kg/m
2. Therefore, Lucy’s postpartum advice should ideally include individualised, goal-driven and BMI-specific weight management advice (
Box 2).
ET
COMPETING INTERESTS: None.
Advertisement
References
1. World Health Organization. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy. Geneva: WHO; 2013.
2. Nankervis A, McIntyre HD, Moses R, et al. for the Australasian Diabetes in Pregnancy Society. ADIPS consensus guidelines for the testing and diagnosis of hyperglycaemia in pregnancy in Australia and New Zealand. 2014. Available online at: http://adips.org/loads/2014ADIPSGDM GuidelinesV18.11. 2014_000.pdf (accessed October 2018).
3. Haertle L, El Hajj N, Dittrich M, et al. Epigenetic signatures of gestational diabetes mellitus on cord blood methylation. Clin Epigenetics 2017; 9: 28.
4. Yan J, Yang H. Gestational diabetes mellitus, programing and epigenetics. J Matern Fetal Neonatal Med 2014; 27: 1266-1269.
5. Australian Government Department of Health Clinical Practice Guidelines: Pregnancy Care. Canberra: Department of Health; 2018.
6. Institute of Medicine. Weight gain during pregnancy: reexamining the guidelines. Washington: National Academies Press (US); 2009.
7. Wong T, Barnes RA, Ross GP, Cheung NW, Flack JR. Are the Institute of Medicine weight gain targets applicable in women with gestational diabetes mellitus? Diabetologia 2017; 60: 416-423.
8. Barnes RA, Edghill N, Mackenzie J, et al. Predictors of large and small for gestational age birthweight in offspring of women with gestational diabetes mellitus. Diabetic Med 2013; 30: 1040-1046.
9. Kim C, Berger DK, Chamany S. Recurrence of gestational diabetes mellitus: a systematic review. Diabetes Care 2007; 30: 1314-1319.
10. Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 2002; 25: 1862-1868.
11. Ehrlich SF, Hedderson MM, Feng J, Davenport ER, Gunderson EP, Ferrara A. Change in body mass index between pregnancies and the risk of gestational diabetes in a second pregnancy. Obstet Gynecol 2011; 117: 1323-1330.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}