Transgender medicine: challenges in personalising care

Gay, lesbian and transgender health
Adolescent health
The demand for transgender medicine and health services is increasing rapidly. However, significant barriers to healthcare exist including stigma, discrimination and lack of medical training in transgender health care. GPs play a crucial role in overcoming these barriers to provide more personalised care for transgender people.
- The GP is the first point of contact for transgender people seeking medical advice.
- A multidisciplinary team (MDT) approach is essential for optimal care of transgender people.
- It is optimal that patients initiating gender-affirming transition should be reviewed by an MDT including an experienced mental health professional and an endocrinologist to recommend, initiate and stabilise appropriate hormonal and psychoactive treatments.
- Once stabilised, ongoing treatment can be provided by the GP with shared-care referral back to the MDT for occasional review and for management problems.
- Creating a welcoming environment provides the first step in increasing access to transgender care.
- Medical and/or surgical therapy, with appropriate monitoring and guidance, aims to improve gender incongruence.
- Preventive medicine with screening for natal organ cancer risk, cardiovascular changes and bone health are essential as part of the long-term care for transgender people.
Gender dysphoria, previously recognised by the American Psychiatric Association in the Diagnostic and Statistical Manual of Mental Disorders (DSM–5), has recently been reclassified in the International Classification of Diseases (ICD-11) under sexual health as ‘gender incongruence of adolescence and adulthood’.1
Mounting evidence suggests that the formation of gender identity involves a complex multidimensional biological cascade not yet well understood.2 In light of these uncertainties, although national and international guidelines are useful to guide the management of gender-incongruent people, it must be kept in mind that they are largely expert opinion, with low levels of evidence, and need to be adapted and implemented for the specific individual.3-6
GPs are the first point of contact for patients seeking medical advice, and transgender individuals are no exception. However, transgender people are often delayed in or precluded from receiving appropriate medical help because of inadequate training, experience and knowledge on the part of the healthcare providers dealing with transgender health.7 This article aims to outline practical steps to help increase adult transgender people’s access to medical care and their comfort with it. It is not meant to be exhaustive, but rather, provides an overview with suggested further reading in this field.
At the consultation room
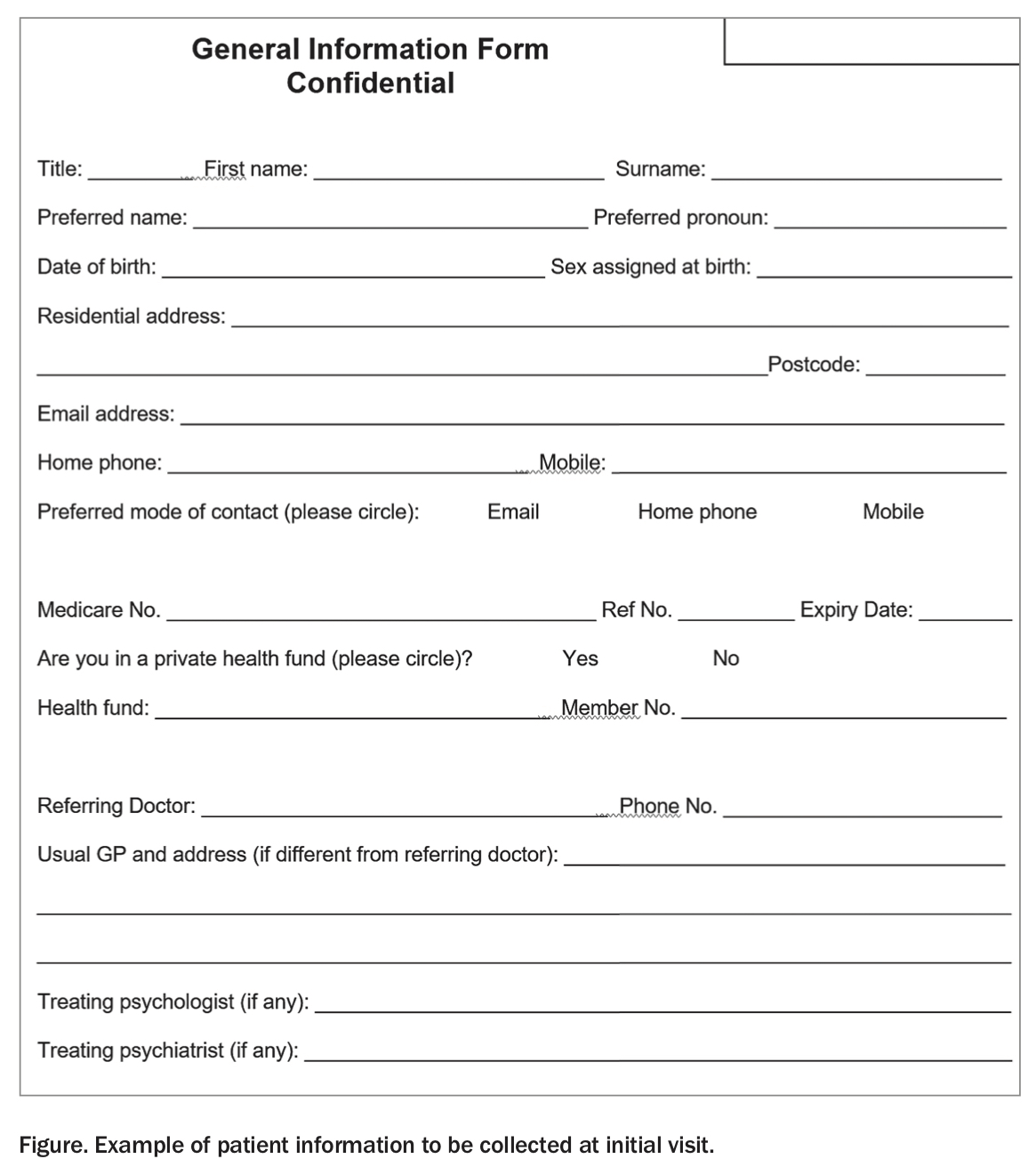
Creating an environment that welcomes everyone is an important first step to keeping individuals, especially new patients, at ease.8 This includes addressing the transgender person by their preferred name and using their preferred gender pronouns in conversations and in the written health record (e.g. he, she, they, them). An example of patient information to be collected is shown in the Figure. Medical personnel including frontline staff should become familiar with the use of appropriate language and terminology and respect confidentiality, as they would for any other patient or would expect for themselves. Provision of gender-neutral bathrooms is ideal.
{kind=link}
Multidisciplinary individual-centred approach
The ideal management approach for transgender individuals is a multidisciplinary team (MDT) with the GP as the primary care provider. It is vital that GPs know when to refer to services including an endocrinologist, psychiatrist, psychologist, sexual health physician, surgeon, nurse specialist and speech pathologist. Unfortunately, some specialists remain uncomfortable or unwilling to accept referrals for transgender people, so keeping an up-to-date list of resources is useful. A list of service providers can be found on the Australian Professional Association for Trans Health website (www.auspath.org). Local Primary Health Networks also provide useful information for GPs.
Initial assessment
A request for gender-affirming treatment can be an opportunity to provide general medical care, including preventive health screening. The general principles of history and physical examination (including documentation and counselling) are similar to those for all other patients of a medical practice. However, there are additional considerations worth noting.
First, it is important that history taking focuses on providing care, rather than on questions to satisfy curiosity. Medical, mental health and surgical history pertinent to transition and medication use are all important parts of initial assessment. After a comprehensive history is taken at the initial visit, it is unnecessary to enquire about sensitive gender-related issues at every subsequent visit, unless medically relevant to that visit. When assessing gender transition, specific history taking can be highly sensitive for the transgender person. Patients are best forewarned with written information, if possible, and the history taking conducted nonjudgmentally. Specific social history, such as behaviour-focused history and counselling about safe sex practices, can be very sensitive but is important. If this is too sensitive for the first visit, it can be done at a later visit when a rapport has been established.
Physical examination is equally important for managing the health of transgender people. The key principle in performing a physical examination in a transgender person is to have an open discussion about what is involved in the physical examination and the rationale for it. Examination of the breasts, genitals or rectum is not routinely required unless there is a clear indication to do so, such as suspicion of undiagnosed gonadal (e.g. Klinefelter’s syndrome) or intersex (e.g. disorders of sexual differentiation) disorders. If these sensitive examinations are necessary, prior explanation should be provided, and examination should proceed with active consent. The presence of a chaperone or support person of the individual’s choice, and delaying examination to later visits are means of alleviating a patient’s anxiety about these examinations.9
Considerations before medical therapy
Not all transgender people desire hormonal therapy to alter their bodies. It is also important to recognise that about 30% of gender diverse people identify themselves as nonbinary.10 Management of these people can be complex and challenging and needs to be individualised, including an awareness of ambivalence and potential regret over irreversible hormonal treatment. Patients need to understand that sex steroid effects on the body cannot be selected for desired effects on some but not other tissues.
When gender-affirming hormonal therapy is desired, the principal goal is to align physical characteristics with gender identity, while managing the potential risks associated with hormone therapy. The main transmasculine hormone therapy is testosterone, and for transfeminine hormone therapy, estradiol is the principal agent. Transgender women often require additional antiandrogens to inhibit testosterone effects when circulating testosterone is not fully suppressed by estradiol.
The importance of a multidisciplinary approach
In the rapidly evolving field of transgender medicine with its limited evidence base, we provide an MDT approach to initiation of gender transition and regard that as an essential starting point for gender-affirming medical care. This includes a comprehensive mental health assessment by a psychologist or psychiatrist with experience in transgender medicine before initiation of hormone treatment. In some cases, this involves a simple evaluation leading to a recommendation of hormonal treatment to alleviate gender incongruence. However, some transgender people have significant mental disturbances, which may be alleviated by transition or may make transition more difficult.
When required, psychotherapy is provided by an experienced mental health professional. The role of a mental health professional is to evaluate psychosocial status and adjustment of the patient, to assist in alleviating gender incongruence and facilitating changes in gender role.
Similarly, we regard it as essential that hormonal therapy be initiated by an experienced endocrinologist, although once established it can continue to be provided by the GP. In most transgender individuals, gender-affirming treatment can then proceed through the GP with shared-care endocrinological review or resolution of problems with hormonal or psychoactive therapies.
Although at present there are limitations on other public-sector MDT facilities for transgender medicine, we believe that at this time such an MDT backdrop for transgender medical care should be a standard that Australian patients should expect and be able to call on in times of need.
The goal of therapy, expectations of physical changes, potential adverse effects and monitoring should be discussed with the individual before initiation of hormonal therapy by the clinician who will prescribe and monitor the therapy. Unsupervised initiation and ongoing use of gender-affirming therapy can be potentially dangerous and is not recommended.
Fertility preservation and family planning should be discussed before medical therapy is started.11 The need for fertility-preserving procedures, which are often invasive and/or costly, has not been well established compared with the option of undertaking conventional artificial reproductive technology procedures if fertility is desired.
Testosterone treatment induces partial hypothalamic-pituitary-ovarian suppression in transgender men. However, this may not provide adequate antiovulatory contraception, so additional advice on reliable contraception is required for transgender men with male partners.12 Transfeminine hormone therapy reduces spermatogenesis, resulting in reduced sperm output as well as impaired sperm motility and fertilising ability.13 Nevertheless, restoration of fertility after cessation of gender-affirming hormone therapy has been reported, and testicular sperm extraction is feasible from retained testes.14 The impact of gender-affirming therapy on fertility has so far only been studied in opportunistic rather than well-designed studies.
Transmasculine therapy
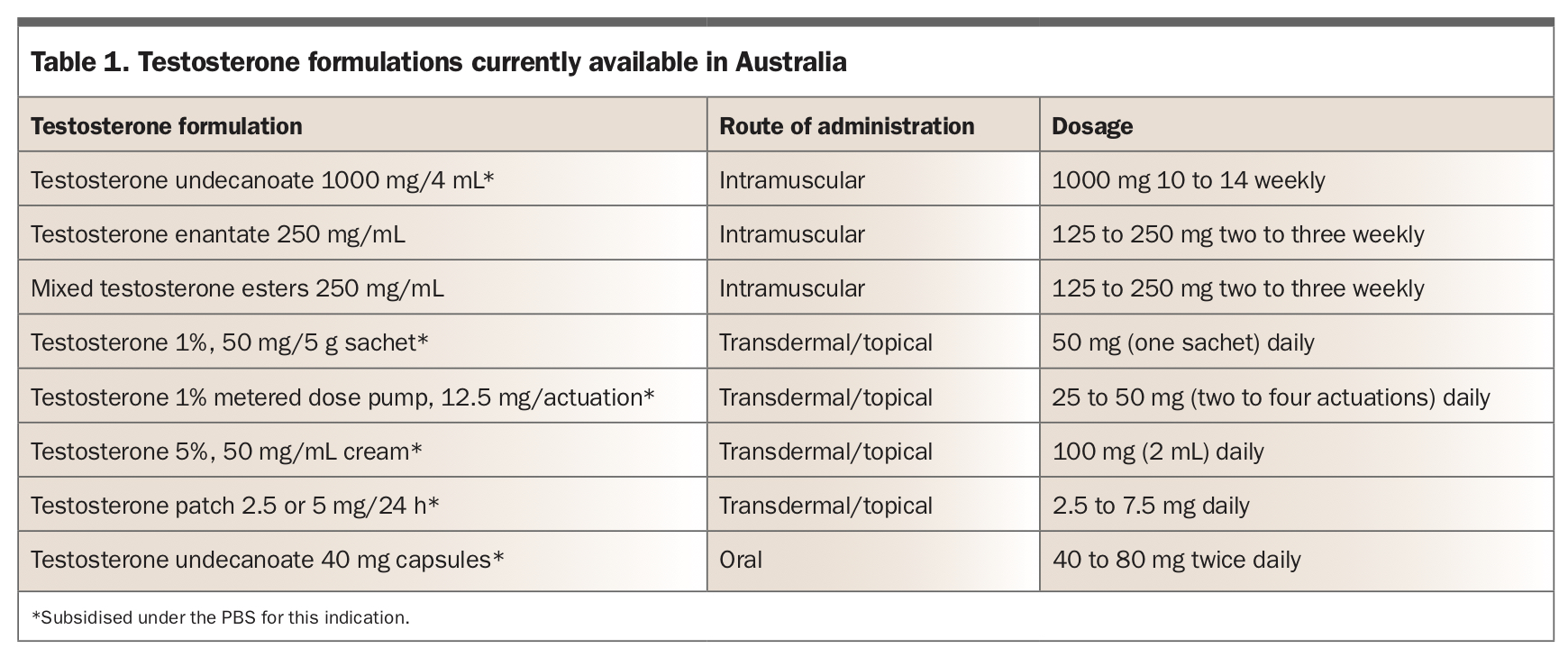
Several guidelines are available for transmasculine therapy with testosterone.3,5,6,15 The testosterone formulations and dosages currently available in Australia are listed in Table 1. In 2015, the criterion ‘male’ required for PBS prescribing was removed so that subsidised testosterone treatment is available for treatment of hypogonadism without regard to natal gender. For transgender men, we use the authority indication ‘androgen deficiency with an established testicular disorder’. For PBS prescription, the patient must be treated by or in consultation with an endocrinologist, paediatrician, urologist or sexual health physician. Ongoing prescription can be provided by the GP by citing the name of the specialist in the authority PBS application. Private non-PBS prescriptions are available at full cost to the patient.
{kind=link}
Testosterone preparations available under the PBS are:
- Testosterone undecanoate 1000 mg (4 mL) intramuscularly, with a loading dose at six weeks, and 12 weekly thereafter, subject to individual titration of the interinjection interval
- Testosterone 1% gel (metered dose pump or sachet) with individual dose titration
- Testosterone 5% cream with individual dose titration
- Testosterone patch 2.5 or 5 mg/24 hours; causes skin irritation and is therefore not popular
- Testosterone undecanoate capsules; requires multiple daily dosing and has low bioavailability.
Outside the PBS, shorter-acting (two- to three-weekly) injectable testosterone esters are available on private non-PBS prescription but are used less often since their removal from the PBS scheme.
Individual dose titration of any testosterone product aims to achieve a trough-level (i.e. at the time of the next scheduled dose) serum testosterone at the lower end of the eugonadal male range (10 to 15 nmol/L).
The physical changes from testosterone have been well described, namely, cessation of menses, development of acne, increased muscle mass and body fat redistribution, deepening of the voice, growth of facial and body hair, balding, clitoral enlargement and changes in body weight.5,16 Deepening of the voice and clitoral enlargement are irreversible and should be clearly explained to the patient before starting treatment. Although individual experience varies, most changes begin within the first three to four months and progress over the first 12 months of testosterone therapy. As with hypogonadal men, subject to careful individual dose titration (and patient tolerance), different testosterone products achieve similar long-term efficacy and physical changes.17,18
Undesirable effects of transmasculine therapy
The risks and side effects of testosterone reflect the known effects of testosterone. Laboratory monitoring for dose titration together with surveillance for adverse effects is performed at baseline and three monthly thereafter for the first 12 months, after which it is required less frequently (e.g. six monthly to annually) unless problems with dosing or adverse effects appear.5
The development of skin changes is common with the use of testosterone.19 One study reported facial acne occurs in at least 80% of individuals at six months of testosterone therapy.20 Acne vulgaris is usually mild and reduces in severity over time.20 Topical therapy with, for example, retinoids, benzoyl peroxide, clindamycin or erythromycin alone or in combination, is often sufficient. Severe changes requiring referral to a dermatologist for specialised treatment (e.g. oral isotretinoin) is uncommon. Testosterone increases circulating haemoglobin and haematocrit in all treated individuals;21 however, clinically troublesome erythrocytosis (i.e. haemoglobin >185 g/L, or haematocrit >0.52) is rare. Significant erythrocytosis is initially managed by reducing testosterone dose (extending injectable dose interval) and, occasionally, by temporarily suspending testosterone or by therapeutic venesection. Smoking cessation is strongly encouraged. Testosterone treatment will usually increase body weight through increased lean (muscle) mass but reduced fat mass. Thus, increased body mass index should not be misinterpreted as increased adiposity.21 In any case, a healthy lifestyle is always recommended.
Transfeminine therapy
Analogous guidelines for transfeminine therapy are also readily available.3,5,6,22 There are different combination regimens, due to prescriber preferences, regional availability and affordability. In principle, the natural steroid estradiol is preferred over synthetic or extracted oestrogens as the major feminising hormone. Estradiol, either orally or transdermally, is the mainstay of feminisation therapy. Although there are no reliable data available on whether transition should be as fast as possible or more gradual, we adopt a gradual transition. Titration of estradiol treatment is primarily based on clinical response, and secondarily on measurement of serum oestradiol (trough level) to avoid supraphysiological levels. Local guidelines, albeit with low quality of evidence, recommend a target trough oestradiol level of between 250 and 600 pmol/L.3
Conjugated estrogens or synthetic oestrogen (e.g. ethinylestradiol) are not recommended given the inability to monitor serum concentration and increased risk of thromboembolic events with these products.23 Oestrogen implants obtained through compounding pharmacies are not recommended due to lack of quality control and unproven safety and efficacy.24
In the absence of bilateral orchidectomy, estradiol alone may not fully suppress circulating testosterone into the normal female or castrate male range (<2 nmol/L). Hence to abolish all androgen action, oestrogen therapy is often combined with antiandrogen therapy. The combination therapies available in Australia are listed in Table 2.
{kind=link}
The two commonly used agents for antiandrogen therapy in Australia are spironolactone and cyproterone acetate. Cyproterone acetate is also a progestin and may affect the mood as well as increase serum prolactin. Serum potassium needs to be monitored when spironolactone is used, as it is a potassium-sparing diuretic as well as an antiandrogen.25 Gonadotropin-releasing hormone agonists are not widely used in Australia (except as Stage 1 pubertal blockade in children and adolescents) due to their cost and limited long-term safety profile in young adults.
Physical changes are generally first evident within two to three months after starting gender-affirming hormone therapy, but progress for two to three years.5 The timeline for these changes is described elsewhere.5,6 The key physical changes include breast development, softening of the skin, mood changes, reduced facial and body hair, reduced sebum production, redistribution of body fat, decreased sexual desire and spontaneous erection, and reduced testicular size.
The addition of progesterone is frequently requested to augment the development of breast tissue. At the time of writing, progesterone is not part of the standard therapy for transgender women. Much inconclusive debate continues regarding this adjunct therapy, especially concerning the use of micronised progesterone.26,27
Undesirable effects of transfeminine therapy
The risk of thromboembolic events in transgender women, especially with oral synthetic or conjugated estrogens, is reported to be between 1 and 5% but is lower for the nonoral route of administration of estradiol.28 Assessment of risk is an important consideration in deciding on the mode and type of oestrogen therapy. Serum prolactin is elevated by oestrogen therapy, and, although prolactinomas are reported in transgender women, causality is doubtful.29,30 Changes in cardiometabolic profile (e.g. lipids, blood pressure, diabetes) are also expected and should be monitored.31
Screening
An important role of a GP caring for transgender individuals is practising preventive medicine. Organ-specific cancer screening is similar to screening among the general population, with individual risk determined by the biological (natal) organs.32 However, putting such screening into effect often requires careful management, as it can increase gender incongruence anxiety in transgender people.33
Patients with a cervix need appropriate screening for cervical cancer risk, including the human papillomavirus screening test. However, cervical examination is often perceived as intrusive and unwelcome among transgender men. As a result, the uptake of cervical cancer risk screening is suboptimal, and much lower among transgender man compared with cisgender women.34
For transgender men who have not undergone bilateral mastectomies, routine breast cancer screening should be conducted as for cisgender women.35 For transgender men who have undergone bilateral mastectomies, there are no breast cancer screening guidelines. It is important to educate patients that breast tissue may not be entirely removed with mastectomy (e.g. preservation of nipple and areolar complex) and that self-examination remains essential. There is no specific guideline for breast cancer screening in transgender women. The current international practice is to recommend that transgender women over the age of 50 years, who have used transfeminine therapy for at least five years, should have screening mammography every two years.33
Routine screening for endometrial and ovarian cancer is not recommended for transgender men.33 Prostate cancer screening comparable with that for the general age-similar population of men should be undertaken.36 For transgender women, the risks and benefits of screening with prostate specific antigen levels with or without digital examination of the prostate should be discussed as it usually would be for any adult man of comparable age.
Sexually transmitted diseases and contraception
Globally, the prevalence of HIV infection is high among the transgender population, especially among transgender women.37 Locally, in Australia, the prevalence of sexually transmissible infections among transgender people remains low.38 Nevertheless, education about safe sexual practice and pre-exposure prophylaxis is paramount. Contraception and pregnancy should also be discussed with all transgender patients.
Cardiovascular metabolic risk factors
Long-term use of gender-affirming hormone treatment, especially transfeminine therapy, is associated with increased cardiovascular risk, most notably with regard to adverse lipid profiles (triglycerides and LDL-cholesterol), and possibly increased incidence of diabetes.31 Screening for these risk factors and encouraging healthy lifestyle modification are as important in the transgender population as they are for the general population.
Bone health
The effects of gender-affirming hormone therapy on bone density are not yet fully elucidated. A key issue is whether bone density should be compared with Z-scores (i.e. age-specific) for cis-male or cis-female normative populations.39 The indication for bone density testing and the interval for repeat testing are additional issues to be individualised in the absence of evidence-based guidelines. Transgender men are reported to have favourable bone mineral density (BMD) compared with cisgender women before therapy, whereas transgender women have lower BMD compared with cisgender men before therapy.39 Therefore, we recommend that reporting of both male and female Z-scores be requested when ordering bone density testing for transgender people. Individuals identified as being at risk of low bone density and fractures should be encouraged to adopt bone health measures including adequate intake of calcium and vitamin D, adequate exposure to sunlight and performing weight-bearing exercise aimed at reducing the risk of osteoporosis and fractures.
Co-ordination of care
Transgender people may require other services including voice training, laser therapy and cosmetic therapy to better align with their desired gender. Moreover, changing legal documentation generally requires reports or a declaration from clinicians. GPs can serve as a key co-ordinator in facilitating these processes.
Conclusion
There is an increasing demand for transgender medicine and health services, and clinicians are encouraged to be familiar with the unique needs of transgender people.40 It is important that all doctors and other medical personnel better equip themselves to understand this population to reduce the barriers to appropriate care. ET