Hormonal contraception: what’s new?

Birth control
Changes in the past 12 months include the PBS listing of a new low-dose levonorgestrel intrauterine device and revised recommendations on placement of the etonogestrel implant, tailored use of combined hormonal contraception, emergency contraception, contraception and vaping, and concurrent use of liver enzyme-inducing medications.
- A low-dose five-year 19.5mg levonorgestrel intrauterine device (LNG-IUD) with a slightly smaller frame than the 52mg LNG-IUD is available on the PBS, offering additional choice of contraception, including for nulliparous and younger people.
- The 52mg, but not the 19.5mg, LNG-IUD inserted at age 45 years or older can be used until menopause is confirmed or age 55 years (off-label extended use).
- The approved placement site for the etonogestrel implant is now over the triceps, about 8 to 10cm from the medial epicondyle and 3 to 5cm below the sulcus, to avoid the risk of damage to large vessels and nerves.
- Extended and flexible use of combined hormonal contraception avoids regular withdrawal bleeding and offers potential benefits in relation to effectiveness and troublesome side effects.
- Australian practitioners need to be aware of contraception methods available in other countries, including the two-rod levonorgestrel implant used in New Zealand.
Shared decision-making about contraception relies on the provision of evidence-informed information. This article provides an update on the range of available hormonal contraception options, including the low-dose 19.5 mg levonorgestrel intrauterine device (LNG-IUD) recently listed on the PBS, as well as new clinical practice guidance on tailored contraceptive pill taking, extended use of IUDs and correct placement of the etonogestrel implant. We also consider contraceptive methods available in other countries that may be encountered in Australia, such as the two-rod levonorgestrel implant used in New Zealand, and new methods under development and regulatory review, which are likely to become available in the future.
In this article, we mostly refer to women to reflect the research evidence on hormonal contraception but acknowledge that trans and gender diverse people also have contraceptive needs.
Update on hormonal intrauterine devices
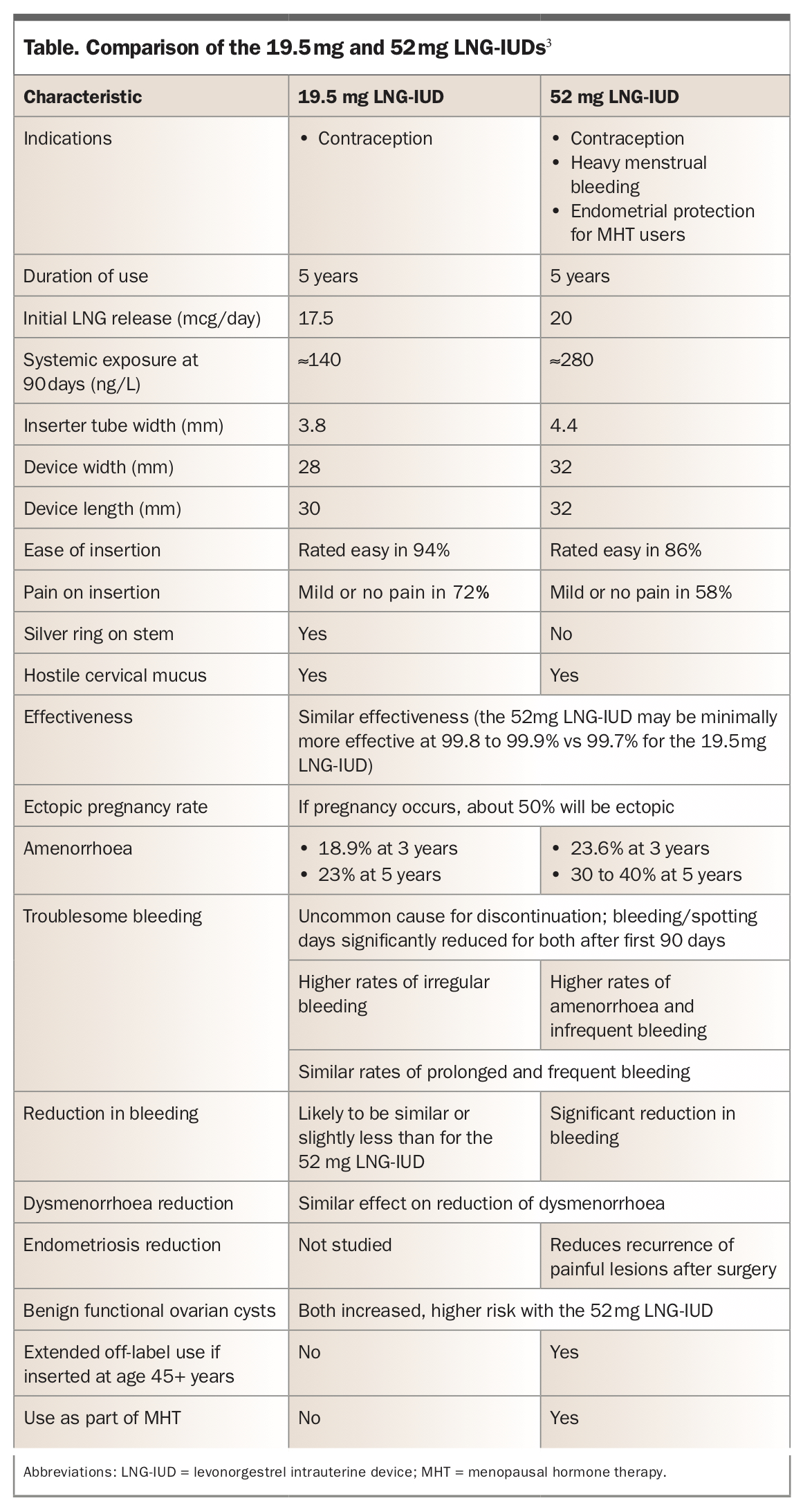
A 19.5 mg LNG-IUD (Kyleena) was listed on the PBS in March 2020. The device is licensed for a duration of five years and is highly effective, at around 99.7% compared with 99.9% for the 52 mg LNG-IUD (Mirena).1-3 A quick comparison between the two LNG-IUDs is available at the Family Planning Victoria website (www.fpv.org.au/assets/img/content/Hormonal-IUDs-available-in-Australia-comparison-chart- for-prescribers-and-IUD-inserters-TOOLS.pdf).4 Important features relevant to GPs are summarised in the Table.3
{kind=link}
The new lower-dose device results in a large reduction in menstrual bleeding in a general population of users.1,2 However, it is not currently indicated for the management of heavy menstrual bleeding, unlike the 52 mg LNG-IUD which has been specifically studied in affected populations.5-8 Overall the number of bleeding or spotting days per month is only slightly less for the 19.5 mg LNG-IUD than for the 52 mg device, but the lower dose LNG-IUD is a little more likely to be associated with irregular bleeding and less likely to be associated with amenorrhoea (a desirable feature for some users).1,9 The 19.5 mg LNG-IUD also reduces dysmenorrhoea in a general population of users, but effectiveness for the management of pain associated with adenomyosis and endometriosis is yet to be proven for the lower dose device.1,3
Other differences between the 52 mg and 19.5 mg LNG-IUDs relate to their use at the perimenopause and menopause. The 52 mg LNG-IUD inserted at the age of 45 years or above can be used for contraception (extended off-label use) until menopause has been confirmed or the woman reaches 55 years of age (see Flowchart).10,11 In contrast, the 19.5 mg LNG-IUD can only be used for a maximum of five years.10,12 Similarly, the 19.5 mg LNG-IUD is not indicated for the progestogenic protection of the endometrium as part of menopausal hormone therapy (MHT). In contrast, the 52 mg LNG-IUD is licensed for this purpose for a maximum of five years of use, with no recommendation for extended use. Note that all the copper-containing IUDs available in Australia, if inserted at the age of 40 years or older, can be used beyond their licensed duration (off-label) until menopause is diagnosed or until contraception is no longer needed.
There are some differences in side effects between the higher and lower dose LNG-IUDs. The 52 mg LNG-IUD and, to a much lesser extent, the 19.5 mg LNG-IUD increase the incidence of ultrasound-detected benign functional follicular ovarian cysts, but their significance is minimal with no evidence of an increased risk of intervention for this condition.1 Despite the systemic exposure to LNG for 19.5 mg LNG-IUD users being about half that of 52 mg LNG-IUD users, limited evidence does not indicate that the lower dose device is associated with fewer general hormonal side effects such as acne and breast discomfort.13 However, studies specifically addressing these issues have not been performed.1
Compared with the 52 mg LNG-IUD, the 19.5 mg LNG-IUD is slightly smaller, may be easier to insert and may be associated with less insertion pain.1 Again, although evidence is lacking for superiority of one device over the other, the smaller size of the 19.5 LNG-IUD may offer an additional suitable choice for nulliparous and younger women. Older women with heavy menstrual bleeding would benefit from the 52 mg device, with greater reduction in menstrual bleeding and extended use at the perimenopause.
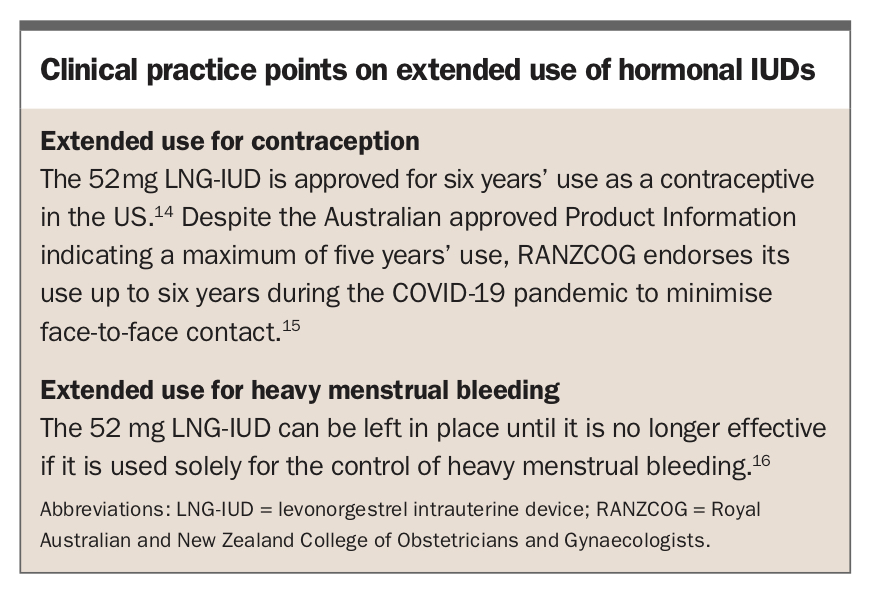
Clinical practice points on extended use of hormonal IUDs are shown in the Box.14-16
{kind=link}
Update on contraceptive implants
The etonogestrel contraceptive implant is highly effective and the most often prescribed long-acting reversible contraception (LARC) method in Australia. Recommendations have changed about the site of placement and about replacement in heavier women.
Site of placement of the etonogestrel implant
There have been a small number of case reports of intravascular insertion resulting in pulmonary artery embolisation of the contraceptive implant.17 An update to the approved Product Information for the etonogestrel implant indicates that the implant must now be inserted over the triceps muscle about 8 to 10 cm from the medial epicondyle and 3 to 5 cm below the sulcus between the biceps and triceps muscles.18 This avoids the large blood vessels and nerves lying within and surrounding the sulcus.19 Replacement implants must be re-sited according to the new recommendations.
Implant replacement in heavier women
The approved Product Information for the etonogestrel implant states, ‘Clinicians may consider earlier replacement of the implant in heavier women’.18 Current Australian advice is that the etonogestrel implant is an effective method of contraception for people who have a raised body mass index (BMI), and that the contraceptive implant should be replaced every three years regardless of BMI.20
Levonorgestrel implants
Australian medical practitioners removing a contraceptive implant that has been inserted in New Zealand and other Pacific countries need to know it is likely to be a two-rod levonorgestrel implant. This implant provides contraception for five years and is available free of charge to New Zealand residents. The single-rod etonogestrel implant is also available in New Zealand but is used infrequently, as the cost to the consumer is around $260.
Levonorgestrel implants are more flexible and fragile than etonogestrel implants. On average they take longer to remove and the procedure is less likely to be rated as easy.21 Both of the rods can usually be removed through a single transverse or longitudinal incision, depending on how close together their proximal ends are located, but occasionally two incisions will be required.
Update on combined hormonal contraception
Tailored pill taking or vaginal ring use
Most combined oral contraceptives (COCs) in Australia are in packs containing 21 days of active hormone pills and seven days of inactive pills, known as the hormone-free interval. Recently more flexible approaches to pill taking have been supported, in that users can either:
- take three months of continuous active pills before a standard or shortened hormone-free interval of seven or four days, or
- take active pills for at least 21 consecutive days until breakthrough bleeding occurs for three to four days, followed by a four-day hormone-free interval before restarting active pills.22
The vaginal ring containing oestrogen and a progestogen can be used in a similar manner, with either:
- a series of three rings used consecutively for three weeks each, followed by a ring-free interval of seven or four days, or
- continuous ring use, with a new ring placed every three weeks, until there are three to four days of breakthrough bleeding, after which the current ring is discarded and a new ring inserted after a four-day break.23
For those who do not get breakthrough bleeding there is no upper limit to the length of time combined hormonal contraception (CHC) can be taken or used without a hormone-free interval. However, annual clinical review is important at the time of a new 12-month prescription.23
Extended CHC regimens are likely to be more effective for contraceptive protection than traditional regimens (with 21 days of active hormones followed by a seven-day hormone-free interval).24,25 Also they may be associated with fewer adverse effects such as headaches, dysmenorrhoea and bleeding, as a result of reduced exposure to hormonal fluctuations during the hormone-free intervals.26
Vaping and combined hormonal contraception
Although the harms of nicotine vaping are considered less than those of smoking in the general population, there are no long-term studies in users of hormonal contraception.27 Until further evidence is available, Australian Family Planning organisations consider vaping with nicotine to be equivalent to cigarette smoking in relation to the medical eligibility criteria for contraceptive use.28 Cigarette smoking at the age of 35 years or above is a relatively strong or absolute contraindication for CHC use if fewer than 15 cigarettes or 15 or more cigarettes, respectively, are smoked per day. Nicotine vaping at any level is an absolute contraindication in this age group.
Update on emergency contraception
The copper IUD is the most effective method of emergency contraception, but the oral methods, ulipristal 30 mg or levonorgestrel 1.5 g, are more often used.29 Ulipristal and levonorgestrel are easy to use and have the convenience of over-the-counter availability at pharmacies. Ulipristal 30 mg, although two to three times more expensive than levonorgestrel 1.5 g, appears to be more effective as emergency contraception and can be used up to five days after unprotected intercourse, compared with four days for levonorgestrel 1.5 mg.30-32 Australian Family Planning organisations have made several new recommendations in relation to oral emergency contraception, which endorse the recommendations of the UK Faculty of Sexual and Reproductive Health, as described below.
A recent study showed lack of inferiority of the 52 mg LNG-IUD compared with a copper TT380 IUD when used for emergency contraception.33 However, the role of the LNG-IUD for this purpose is yet to be determined.
Ulipristal and breastfeeding
Product Information indicates breastfeeding is not recommended for one week after taking ulipristal acetate.34 However, current Australian recommendations state that breastfeeding can be continued uninterrupted, as the risk to the infant is low. Those wishing to avoid the highest levels of infant exposure can be advised to express and discard breast milk for 24 hours after taking ulipristal.35
Ulipristal and other hormonal contraception
Two studies have shown that if progestogen-containing contraception is started soon after taking ulipristal 30 mg, the efficacy of ulipristal might be reduced.36,37 It is currently recommended that initiating or restarting combined hormonal contraception, the progestogen-only pill, etonogestrel implant or depot medroxyprogesterone acetate injection should be delayed for five days if ulipristal 30 mg is used for emergency contraception. This advice does not apply to the LNG-IUDs because of the low systemic levels of LNG and because the progestogen is acting mainly at a local rather than systemic level.35
Theoretically, progestogen-containing contraception taken before the use of ulipristal 30 mg might also diminish the efficacy of ulipristal as emergency contraception. However, there is no supportive clinical evidence of this effect. If hormonal contraception (excluding LNG-IUDs) has been used in the week before emergency contraception is required, and a copper IUD is not suitable, then levonorgestrel emergency contraception can be considered as an alternative to ulipristal.29,35
Emergency contraception and body weight
The efficacy of oral emergency contraception may be affected by body weight.38 In situations where a copper IUD is not appropriate, a double dose of levonorgestrel is recommended for those with a BMI greater than 26 kg/m2 or weighing more than 70 kg.
The efficacy of ulipristal might also be reduced in those with a BMI greater than 30 kg/m2 or weight greater than 85 kg, but there is no recommendation for a double dose of ulipristal. Evidence is lacking for superiority of either a double dose of levonorgestrel emergency contraception or a single dose of ulipristal in this context.29
New recommendations for liver enzyme-inducing medications
Liver enzyme-inducing medications, including some antiepileptics, modafinil and the over-the-counter preparation St John’s wort, have the potential to reduce the efficacy of CHCs, the progestogen-only pill, the contraceptive implant and oral emergency contraception. The depot medroxyprogesterone acetate injection and LNG-IUDs are unaffected and are the methods of choice in concurrent users of liver enzyme-inducing medications.
Comprehensive advice is available from the UK Faculty of Sexual and Reproductive Health.39 Australian Family Planning organisations have released two recent changes to practice regarding topiramate and griseofulvin, as follows.
- Topiramate. The liver enzyme-inducing medication topiramate was previously considered to affect contraceptive efficacy only at doses of 200 mg or above. It is now considered to reduce the efficacy of affected hormonal contraceptives at any dose.40
- Griseofulvin. Although griseofulvin is not a liver enzyme-inducer, there have been case reports of contraceptive failure and menstrual disturbance in users.41-43 Because of the potential for teratogenicity, griseofulvin is treated in the same manner as liver enzyme-inducing medications in users of hormonal contraception.39,44,45
Recommendations for stopping contraception at menopause
Bleeding patterns cannot be relied on to diagnose menopause in users of hormonal contraception. CHC methods should not be continued beyond 50 years of age, and the depot medroxyprogesterone acetate injection should be stopped at this age in most circumstances.39 Generally, it is recommended that women switch to a contraceptive implant, progestogen-only pill, hormonal or copper IUD or a barrier method until menopause can be determined or the age of 55 years, when the chance of conception is extremely low even in menstruating women. Advice on managing contraception in those aged 50 years or over, including the use of a single FSH level in progestogen-only contraceptive users with amenorrhoea, is shown in the Flowchart.
Contraceptive methods in development or available in other countries
Oral drospirenone progestogen-only pill
A drospirenone (4 mg) progestogen-only pill was recently approved for use in the US. This new pill, packaged with 24 active tablets and four inactive tablets, has several of the advantages of COC pills without the contraindications and risks related to oestrogen use. It acts primarily by stopping ovulation and appears to have similar efficacy to COC pills and an acceptable bleeding pattern. It is considered safe to use during lactation and immediately after delivery. Most importantly, it has a 24-hour timeframe for administration, unlike the current low-dose progestogen-only pills available in Australia, which must be taken within a narrow three-hour window each day to maintain efficacy.46
A desogestrel (75 mcg) progestogen-only pill is available in several countries, including New Zealand. This pill also causes anovulation, is taken continuously without a hormone-free interval and has a 12-hour rather than 24-hour timeframe for administration.47
Combined hormonal pill with estretol in place of ethinylestradiol
Estetrol (E4) is a natural oestrogen, present only during pregnancy and shortly after birth. Estetrol chemically synthesised from estrone has recently gained attention for its use in CHC, with an estetrol and drospirenone combined hormonal pill currently under regulatory review by the US Food and Drug Administration.48 Early studies indicate its use is associated with high efficacy and acceptable bleeding patterns. Other evidence indicates a lower impact on markers of haemostasis compared with currently available combined hormonal pills, which may translate into safety benefits in relation to deep vein thrombosis.49
New combined hormonal vaginal ring
A vaginal ring releasing ethinylestradiol and a novel progestogen, segesterone acetate, has been released in the US. Segesterone binds selectively to progesterone receptors to block ovulation without the androgenic and estrogenic impacts seen with other progestogens.The ring can be used for up to 12 months and does not require refrigeration. It is left in place for 21 days, then temporarily removed and reinserted after seven days.50
Self-administered subcutaneous depot medroxyprogesterone acetate
A self-administered three-monthly subcutaneous depot medroxyprogesterone acetate product is available in several countries. Self-injection is acceptable to most users and convenient, as a 12-month supply can be kept at home.51,52 It may also have benefits for those using anticoagulants and for those with obesity, for whom subcutaneous administration is more easily achieved than intramuscular injection.
Conclusion
The increasing array of contraceptive choices and evidence-informed clinical practice updates help support every person requiring contraception to find a method that best suits their individual needs. The role of the clinician is to provide the most up-to-date information to support informed decision-making and to practise in a person-centred manner, while adhering to current best-practice guidelines. ET