Established CVD in people with type 2 diabetes: what pharmacotherapy should be considered?

Diabetes type 2
The results of recent cardiovascular outcome studies have significantly influenced pharmacotherapeutic recommendations for patients with type 2 diabetes who have established cardiovascular disease or risk factors. The new advice is that sodium-glucose cotransporter-2 inhibitors or glucagon-like peptide-1 receptor agonists should be considered on top of standard care. However, the importance of achieving glycaemic targets remains, and the patient’s GP and other members of the patient’s diabetes team also need to address other complications of diabetes.
- The management of type 2 diabetes requires that cardiovascular risk factors are addressed. Lifestyle advice, smoking cessation counselling and appropriate pharmacotherapy to attain glycaemic, lipid and blood pressure targets are all essential.
- The results of recent cardiovascular outcome studies have significantly influenced pharmacotherapeutic recommendations.
- Consensus recommendations from the American Diabetes Association and European Society for the Study of Diabetes indicate that in high-risk individuals, a glucagon-like peptide-1 receptor agonist (GLP-1 RA) or sodium-glucose cotransporter-2 (SGLT-2) inhibitor should be considered, GLP-1 RAs should also be considered in patients with type 2 diabetes without established cardiovascular disease (CVD) but with the presence of specific indicators of high risk, and SGLT-2 inhibitors are recommended in patients with type 2 diabetes and heart failure as well as in patients with type 2 diabetes with chronic kidney disease.
- The Australian Diabetes Society type 2 diabetes treatment algorithm also indicates that the choice of agents should be guided by clinical considerations (e.g. the presence of CVD).
- The use of these newer agents and their potential benefits does not negate the importance of setting and achieving appropriate glycaemic targets.
- When these agents are used, a detailed discussion about the potential benefits and also the potential side effects is required.
Diabetes is the fastest growing chronic illness in Australia, with two-thirds of all deaths in people with diabetes due to cardiovascular disease (CVD). CVD, which is atherosclerotic in origin, is defined as established coronary heart disease, cerebrovascular disease or peripheral arterial disease.1 Other cardiometabolic risk factors such as hypertension, dyslipidaemia, obesity and smoking are often comorbidities in diabetes.1 Heart failure is a frequent but sometimes forgotten manifestation of CVD.2 This article focuses on diabetes medications to be considered when there is established CVD in patients with type 2 diabetes; however, other complications and associations of diabetes such as renal disease, retinopathy, neuropathy, depression and cognitive impairment will also need to be addressed by the GP and other members of the diabetes team.
What has been known previously?
In terms of prevention and management of CVD, risk factors such as obesity/overweight, hypertension, dyslipidaemia, smoking, chronic kidney disease and the presence of albuminuria should be assessed in every patient.1
The use of statin therapy, renin-angiotensin system blockade for hypertension and smoking cessation with counselling and/or pharmacotherapy are all well-established standard interventions. Addressing multiple risk factors has also been demonstrated to be of benefit in decreasing cardiovascular complications in patients with type 2 diabetes.3
Blood pressure targets should be individualised but, in general, a systolic blood pressure of less than 130 to 135 mmHg is reasonable.4,5 Pharmacotherapy should include ACE inhibitors or angiotensin II receptor blockers (ARBs) but other agents such as thiazides or calcium channel blockers may also be needed. In the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial, blood pressure targets of less than 140/90 mmHg were found not likely to improve cardiovascular outcomes in people with type 2 diabetes with established CVD, so the old teaching of ‘lower is better’ may not hold.6
With regard to lipid management in diabetes, the American Heart Association guidelines indicate that, in terms of ‘primary prevention’, moderate-intensity statin therapy (e.g. atorvastatin 10 to 20 mg daily, rosuvastatin 5 to 10 mg daily, simvastatin 20 to 40 mg daily or pravastatin 40 to 80 mg) is recommended in patients 40 to 75 years of age without clinical atherosclerotic CVD.7 In those with multiple cardiovascular risk factors or aged 50 to 70 years, the use of high-intensity statin therapy (e.g. atorvastatin 40 to 80 mg daily or rosuvastatin 20 to 40 mg daily) is recommended. In terms of ‘secondary prevention’, for people of all ages with diabetes and CVD, high-intensity statin therapy should be used. These recommendations contrast with the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) guidelines that aim for LDL-cholesterol (LDL-C) targets. These include: treatment for primary or secondary prevention in those at very high risk; a therapeutic regimen that achieves an LDL-C reduction equal to or greater than 50% from baseline and LDL-C levels less than 1.4 mmol/L. In those at high risk, the recommended targets are an LDL-C reduction equal to or greater than 50% from baseline and an LDL-C level less than 1.8 mmol/L. The ESC/EAS cardiovascular risk categories are shown in the Table.8
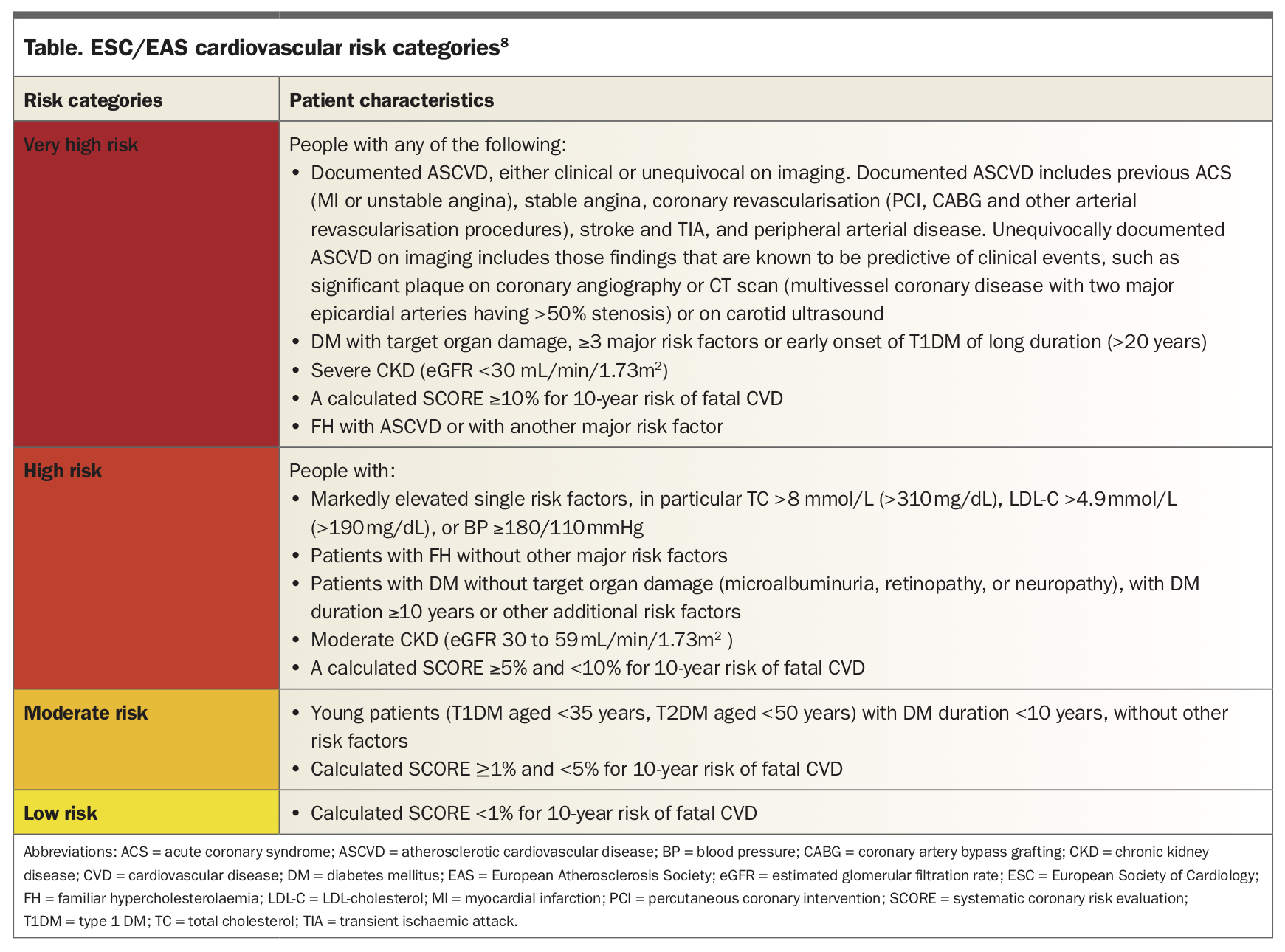{kind=link}
Low-dose aspirin should be used as a secondary prevention therapy in those with diabetes and history of atherosclerotic CVD. A discussion needs to occur with the patient regarding potential benefits versus bleeding risk.9,10
The results of the UKPDS (United Kingdom Prospective Diabetes Study) have indicated that in those with newly diagnosed diabetes, achieving a median HbA1c of 7% in the ‘intensive’ group compared with 7.9% in the ‘conventional’ group over 10 years could translate to lower longer-term cardiovascular complications – the so-called ‘legacy effect’.11 However, if there is established CVD or a long duration of diabetes, there may be no benefit and potentially harm when there are rapid decreases in blood glucose and HbA1c levels, and a gradual individualised approach to glucose lowering as seen in the ADVANCE (Action in Diabetes and Vascular Disease Preterax and Diamicron MR Controlled Evaluation) trial may be more appropriate.12,13
What is the effect of antihyperglycaemic agents?
Metformin has been a long-standing first-line therapy for diabetes, with some evidence that it may be beneficial in terms of cardiovascular outcomes (shown in a small subset of overweight/obese patients in the UKPDS).11
There has been inconsistency and controversy regarding the cardiovascular safety of sulfonylureas, which may be related to the type of sulfonylurea used. Some studies have been supportive of the cardiovascular safety of this class.14,15 However, there was no dedicated cardiovascular outcome study (CVOT) until the recent CAROLINA (Cardiovascular Outcome Study of Linagliptin versus Glimepiride in Patients with Type 2 Diabetes), which demonstrated noninferiority of glimepiride compared with linagliptin on major adverse cardiovascular outcomes, although the rates of hypoglycaemia were higher in those taking glimepiride.16 In addition, the use of gliclazide (which has not been marketed in the US where CVOTs are mandatory) in the ADVANCE study was not associated with any adverse cardiovascular outcomes, with an improvement in microalbuminuria – a marker of cardiovascular risk – although this may have related to the improvement in glycaemic control.12
Dipeptidyl peptidase-4 (DPP-4) inhibitors are generally regarded as ‘safe’ and have a neutral effect on cardiovascular outcomes, with none of the trials showing an increase in major cardiovascular events (3-point MACE; cardiovascular death, nonfatal myocardial infarction and nonfatal stroke), although there is no CVOT evaluating vildagliptin, which is also not marketed in the US.17-21 However, it should be noted that there was a small increase in the number of hospitalisations for heart failure with saxagliptin (0.7%), particularly for patients at the highest absolute risk of heart failure in the SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus-Thrombolysis in Myocardial Infarction 53) study.21
What has changed?
The American Diabetes Association (ADA) and European Association for the study of Diabetes (EASD) consensus report, initially published in 2018 and updated in 2019, has potentially changed the way in which we may select pharmacological therapy in type 2 diabetes in those with established CVD.22 These recommendations are based on the results of CVOTs. The consensus recommendation was that in the setting of type 2 diabetes, established CVD was a compelling indication for treatment with a glucagon-like peptide-1 receptor agonist (GLP-1 RA) or sodium-glucose cotransporter-2 (SGLT-2) inhibitor. Moreover, the recommendation was that in ‘appropriate high-risk individuals’ with established CVD, the use of these agents should be considered independently of baseline HbA1c levels or the HbA1c target level for the individual.22
It should be noted that, in Australia, the TGA indication and/or PBS criteria for subsidy for antihyperglycaemic medications will have a substantial role in determining which medication or combinations of medications may be used. The recently updated Royal Australian College of General Practitioners and Australian Diabetes Society guidelines reflect this.23,24
The above studies have indicated potential reno-protective effects of SGLT-2 inhibitors.
Sodium-glucose cotransporter-2 inhibitors
SGLT-2 inhibitors have potential beneficial effects on cardiovascular risk factors and cardiorenal disease, including a decrease in HbA1c levels, blood pressure and weight.1,25 In the CVOTs, use of these agents has been associated with reductions in cardiovascular morbidity and, in the case of EMPA-REG Outcome ([Empagliflozin] Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients-Removing Excess Glucose), cardiovascular mortality.25 Benefits appear independent of glycaemic control. These agents include dapagliflozin, empagliflozin, ertugliflozin and canagliflozin (the last is no longer available in Australia).
In the EMPA-REG Outcome – in which more than 99% of participants had established CVD – there was a statistically significant 14% relative risk reduction in 3-point MACE outcomes in those randomised to empagliflozin compared with placebo, with the reduction primarily due to cardiovascular-related death (38% relative risk reduction) as well as a 35% decrease in the risk of hospitalisation for heart failure.25
In the DECLARE (Dapagliflozin Effect on Cardiovascular Events)-TIMI [thrombolysis in myocardial infarction] 58 trial – in which there were participants with and without established CVD – there was no statistically significant reduction in 3-point MACE outcomes in patients randomised to dapagliflozin, although there was a statistically significant reduction in the combined endpoint of cardiovascular death (4.9%) or hospitalisation for heart failure (5.8%) – largely due to the decrease in hospitalisation for heart failure.26
In CANVAS (Canagliflozin Cardiovascular Assessment Study), there was a statistically significant 14% reduction in MACE outcomes with the use of canagliflozin compared with placebo and a decrease in hospitalisation for heart failure.27 A meta-analysis of these three studies showed that in patients with established atherosclerotic CVD, use of SGLT-2 inhibitors was associated with a reduction in 3-point MACE.28 More recently, the results of VERTIS-CV (Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial) – in which participants had established CVD – showed a decrease in hospitalisation for heart failure and noninferiority compared with placebo for cardiovascular events in those randomised to ertugliflozin.29
The treatment algorithm of these guidelines indicates that the choice of medication should be guided by clinical considerations such as the presence of CVD, heart failure or renal disease. There are a number of studies specifically evaluating the effects of SGLT-2 inhibitors and renal disease, including the CREDENCE (Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy) trial, in which the benefits of SGLT-2 inhibitors on progression of diabetic renal disease (end-stage kidney disease, a doubling of the creatinine level or death from renal cause) was shown.30 There are other studies underway.
It may not be possible to accurately directly compare the effects of the different SGLT-2 inhibitors as they were studied in different clinical trials. However, a consistent finding across the trials has been the significant decrease in heart failure hospitalisations in patients treated with SGLT-2 inhibitors on top of usual care regardless of established CVD. There are variable but, at minimum, neutral effects on MACE outcomes (positive in the EMPA-REG OUTCOME and CANVAS studies) and, in those with established CVD, a decrease in cardiovascular death in the EMPA-REG Outcome.
In Australia, the TGA indication for empagliflozin includes an indication to reduce the risk of cardiovascular death in people with type 2 diabetes and established CVD, whereas the TGA indication for dapagliflozin includes an indication to decrease the risk of hospitalisation for heart failure in patients with type 2 diabetes and established CVD or cardiovascular risk factors.
Currently, SGLT-2 inhibitors in Australia are indicated for initiation in those with an estimated glomerular filtration rate (eGFR) greater than 45 mL/min/1.73m2 and should be discontinued if the eGFR is less than 30 mL/min/1.73m2 or persistently between 30 and 45 mL/min/1.73m2 due to lesser glycaemic efficacy at lower renal function. However, the results of studies specifically in patients with renal disease may further guide therapy in the future. There should be a detailed discussion with patients about the potential benefits but also about the precautions needed when using this class of agents. Discussion points include increased urinary frequency, a potential decrease in blood pressure and an increased risk of mycotic infections, particularly genital but also urinary tract infections. Patients need to be informed of the rare but important increased risk of euglycaemic ketoacidosis. This can be minimised through education on the risks of fasting, low carbohydrate diets and dehydration. Patients should be also advised to temporarily cease medication during illness and three days before surgery or other procedures.31
Glucagon-like peptide-1 receptor agonists
GLP-1 RAs have clinical benefits such as decreases in HbA1c levels, weight loss and reduction in blood pressure. Currently available therapies in Australia on the PBS are exenatide (immediate release or long-acting weekly) dulaglutide and semaglutide. Liraglutide is available on a private prescription.
The REWIND (Researching Cardiovascular Events with a Weekly Incretin in Diabetes) study – which evaluated the safety of once-a-week dulaglutide versus placebo in patients with and without established CVD – showed a statistically significant 12% reduction in MACE outcomes in those randomised to dulaglutide. Notably, these effects were seen in those with no history of CVD but who had multiple cardiovascular risk factors (69% of the study population), as well in those with established CVD.32
In EXSCEL (Exenatide Study of Cardiovascular Event Lowering Trial) – with exenatide in the extended release once-weekly injection versus placebo – exenatide was found to be noninferior to placebo in terms of MACE outcomes, with no statistically significant reduction, although there has been considerable comment about the design of the study.33 The study had a pragmatic design; its population was broad and included participants at any level of cardiovascular risk, it had no run-in period and the number of premature discontinuations of treatment was high.
In the SUSTAIN-6 (Efficacy and Safety of Once-weekly Semaglutide Monotherapy Versus Placebo in Patients with Type 2 Diabetes) trial there was a decrease in MACE outcomes in those randomised to semaglutide.34 The number of participants was lower compared with REWIND and EXSCEL, and included those at high cardiovascular risk or with established CVD. The primary hypothesis of noninferiority of semaglutide compared with placebo was confirmed, with a statistically significant 26% reduction in the primary outcome of cardiovascular death, nonfatal myocardial infarction or nonfatal stroke.
In the LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial there was a statistically significant reduction in MACE outcomes in patients randomised to liraglutide (13%), particularly a significant reduction in deaths from cardiovascular causes (22%).35 In this study, 81% of the participants had established CVD.
It also may not be possible to accurately directly compare the effects of the different GLP-1 RAs as they were studied in different clinical trials. However, the CVOTs involving the more ‘potent’ agents have demonstrated cardiovascular benefits mainly related to MACE outcomes; a decrease in the incidence of stroke demonstrated in the REWIND and SUSTAIN-6 trials are now being actively explored, as well as potential renal benefits.36
In Australia, the TGA indication for liraglutide includes an indication to decrease cardiovascular events in those with high cardiovascular risk. The TGA indication for dulaglutide includes an indication as an adjunct to standard of care therapy in adults with type 2 diabetes who have established CVD or multiple cardiovascular risk factors, to reduce the risk of major adverse cardiovascular events.
Nausea, vomiting and other gastrointestinal side effects are the most common side effects of GLP-1 RA initiation but are usually self-limiting. It should also be noted that there was a small increase in retinopathy (those requiring photocoagulation or intravitreal injections, as well as vitreous haemorrhage or diabetes-related blindness) in the SUSTAIN-6 trial evaluating the safety of semaglutide, although this is likely due to the rapid glucose lowering in people with known retinopathy rather than a drug-specific effect.
It is intriguing to consider whether the combination of an SGLT-2 inhibitor and a GLP-1 RA might be beneficial. These agents have additive effects on HbA1c levels and weight gain but currently no CVOTs are planned using the combination.37,38 The use of these agents is also limited by PBS guidelines.
Conclusion
Diabetes management is changing and there is now a more targeted approach to address specific complications as well as glycaemic control. In addition to the usual management of cardiovascular risk factors in people with diabetes, identifying those with established CVD and choosing a glycaemic agent that also has nonglycaemic benefits should be strongly considered.
The ADA-EASD consensus statement recommends that an SGLT-2 inhibitor or a GLP-1 RA should be considered in patients who are at high risk or who have established CVD, and a GLP-1 RA where there may not be established CVD but where there are multiple risk factors. In patients with diabetes and concurrent heart failure, SGLT-2 inhibitors would be an appropriate choice. It is apparent that these agents have nonglycaemic effects which result in cardiorenal benefits. At the time of writing, studies evaluating the effects of SGLT-2 inhibitors in patients with and without diabetes have also indicated benefits of these agents in heart failure and renal disease.39-41 Studies are also underway evaluating the effects of GLP-1 RA on renal disease and stroke.
The potential for cardiovascular and renal protection is exciting. However, the importance for cardiorenal protection does not negate the responsibility of the diabetes team to optimise glycaemic control, which has significant effects not only on macrovascular but also microvascular and neuropathic complications as well as ensuring that the use of these newer agents is appropriate for the patient. ET