Atypical femur fractures: the need for timely diagnosis and intervention

Fractures
Osteoporosis
Antiresorptive drugs, namely bisphosphonates and denosumab, are effective therapies for osteoporosis; however, atypical femur fractures have emerged as rare adverse events associated with use of antiresorptive drugs. Atypical femur fractures are associated with significant morbidity and clinician awareness is important for timely diagnosis and intervention.
- Atypical femur fractures (AFFs) are rare spontaneous femur fractures linked to prolonged antiresorptive therapy for osteoporosis.
- AFFs are associated with significant morbidity, delayed healing and prolonged immobilisation. They may also be bilateral.
- Thigh or pelvic pain in a patient taking antiresorptive drugs is a red flag that requires further radiological assessment (plain x-ray, bone scan, MRI or CT) to exclude AFFs.
- Management of AFFs requires multidisciplinary specialist input and includes cessation of antiresorptive drugs and consideration of surgical intervention.
- Despite the significant impact of AFFs for the individual, the burden of ‘typical’ osteoporotic femur fractures remains 50- to 100-fold higher than AFFs. Given the large number of other fragility fractures potentially prevented, the benefit to risk ratio remains strongly in favour of initiating antiresorptive therapy in older adults with osteoporosis.
Osteoporosis and osteopenia affect 4.7 million people in Australia and are associated with significant morbidity and mortality, with the burden expected to rise with an ageing population.1 Antiresorptive drugs, both oral or intravenous bisphosphonates and denosumab, reduce the risk of fractures by up to 70%.2 However, atypical femur fractures (AFFs) have recently emerged as rare adverse events associated with the use of antiresorptive drugs.3,4 This has led to clinician and patient concern over the use of these effective osteoporosis therapies, with an overemphasis of this rare adverse event linked to a decline in uptake of osteoporosis drugs.5
This article aims to raise awareness of these rare fractures and provides guidance on the screening and treatment of AFFs, as well as balanced evidence on the risks and benefits of antiresorptive agents (bisphosphonates and denosumab).
Definition of atypical femur fractures
AFFs have unique radiological features (Figures 1a and b) that distinguish them from a ‘typical’ subtrochanteric or diaphyseal femur fracture (Figures 2a and b).4 AFFs are located in the subtrochanteric or diaphyseal region of the femoral shaft, originate from the lateral aspect of the femur and are predominantly transverse in nature, but may become oblique as they progress medially. AFFs are minimally comminuted or noncomminuted and can be associated with lateral ‘cortical beaking’. The features needed to satisfy a definition of AFF are outlined in Box 1.
{kind=link}
{kind=link}
{kind=link}
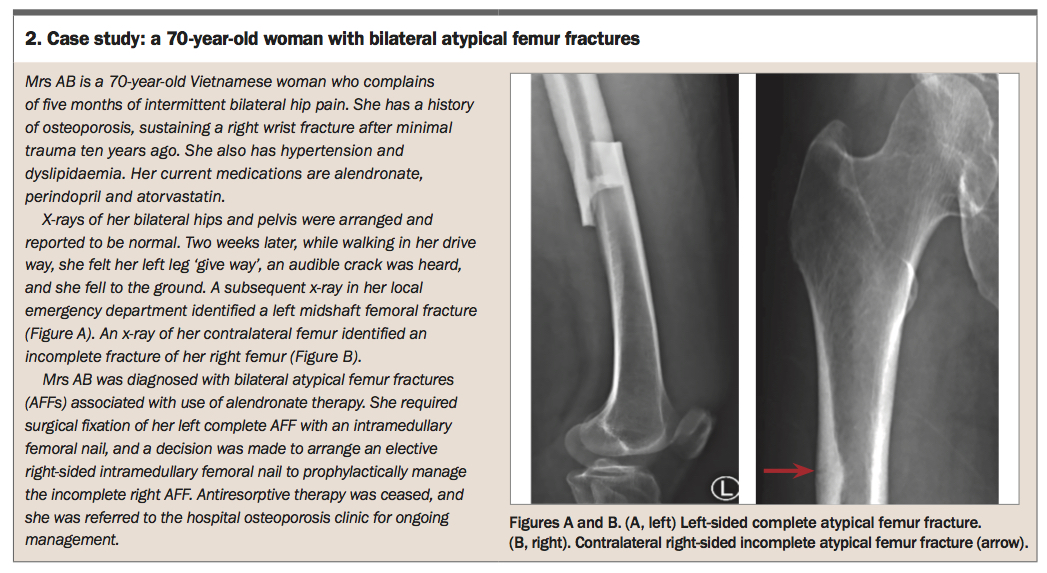
Complete AFFs involve a fracture line that extends through the entire femoral shaft, whereas incomplete AFFs originate from the lateral femoral cortex and do not extend across the entire shaft. Patients may report prodromal thigh pain, which can occur in up to 70% of cases, representing an incomplete AFF. This can progress to a complete fracture either occurring spontaneously or in the setting of minimal trauma (see the Case Study in Box 2).
{kind=link}
Association with antiresorptive therapy
The underlying pathogenesis of AFFs is not completely understood, with the link between AFFs and antiresorptive therapy being paradoxical, as the purpose of these agents is to prevent fractures. It has been proposed that prolonged antiresorptive drugs alter the biomechanical properties of bone, with over-suppression of bone remodelling allowing microdamage to accumulate.6 Weightbearing on these bones with microdamage leads to increased biomechanical strain, particularly affecting the lateral aspect of the femur shaft at the site of maximal biomechanical force. With repetitive loading, stress fractures occur and progress to complete AFFs.
Clinical risk factors
Antiresorptive therapy remains the strongest risk factor for developing an AFF, with up to 90% of AFF cohorts reporting prior use.7 However, several other clinical risk factors have also been described. These include relatively younger age than patients who sustain typical osteoporotic hip fractures, higher body mass index, Asian ethnicity, rheumatoid arthritis, diabetes mellitus and use of other concomitant drugs, such as glucocorticoids, statins and proton pump inhibitors.6 Underlying monogenetic conditions, such as hypophosphatasia, osteogenesis imperfecta and pycnodysostosis, have also been linked to AFFs.8
Balancing the risks and benefits of antiresorptive drugs
AFFs are rare, with a cumulative incidence of three AFF cases per 100,000.7 However, the incidence increases with prolonged antiresorptive drug use, such that more than eight years of exposure to bisphosphonate therapy was associated with an AFF incidence rate of 113.1 per 100,000 person-years.7
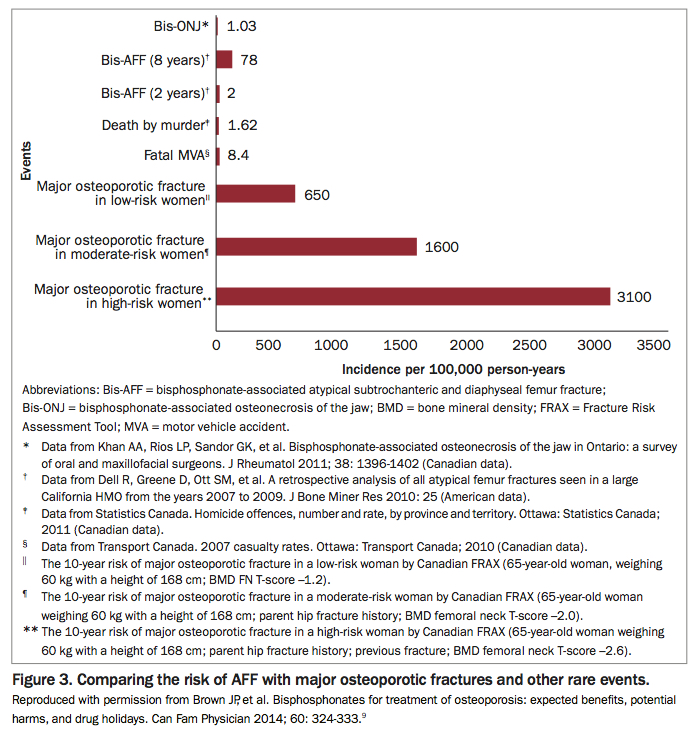
AFFs are exceedingly rare compared with other major osteoporotic fractures (Figure 3).9 A recent audit at our institution confirms that the incidence of AFF in an Australian population is low, with the risk of ‘typical’ hip fractures 50-fold higher than that of AFFs (unpublished data). As such, the benefits of antiresorptive therapy to prevent fragility fractures in people with osteoporosis far outweigh the risk of AFFs. Clinicians should remain confident in initiating antiresorptive drugs in patients with osteoporosis at high risk of fragility fracture. This is particularly important because, unfortunately, undertreatment of osteoporosis remains common.10
{kind=link}
Recent guidelines have provided recommendations on the optimal duration of bisphosphonate treatment to mitigate the risk of this rare complication associated with prolonged use.11 In contrast, there are no guidelines on the optimal duration of denosumab therapy and ‘drug holidays’ are not recommended for this antiresorptive therapy because of its rapid offset of action.
In patients who are at low risk of fragility fracture, after three to five years of bisphosphonate drug use, clinicians may consider recommending a ‘drug holiday’ from bisphosphonate therapy for two to three years. It is important to continue to monitor bone density during a ‘drug holiday’, as osteoporosis treatment may need to be recommenced in the setting of a decline in bone density or a new fragility fracture.
In patients at high risk of fragility fractures, continuing bisphosphonate treatment for up to 10 years has been shown to reduce the risk of fragility fracture. Therefore, antiresorptive therapy should be continued in patients at high risk of fragility fractures.
Diagnosis of atypical femur fractures
Complete AFFs can lead to significant morbidity, delayed healing, and prolonged immobilisation.4 Early detection of an incomplete AFF may allow intervention before the fracture becomes complete. Patients on antiresorptive drugs should be routinely asked about hip, groin or thigh pain, which usually worsens with weightbearing. Pain in these regions should prompt the clinician to consider AFFs, and further imaging arranged to exclude an incomplete AFF.
Bilateral hip and full-length femur x-rays are useful in assessing for lateral femoral cortical beaking and presence of a fracture line. The x-ray should be reviewed carefully to assess for major criteria for AFF, as outlined in Box 1. It is particularly important to state the history of bisphosphonate use and thigh pain on the radiology request and raise the concern of possible AFFs, so that radiologists can carefully review the x-rays in this context. If detected, imaging of the contralateral femur is necessary to exclude contralateral AFFs, as bilateral AFFs occur in up to 40% of cases.
In the setting of hip or thigh pain, if x-rays cannot detect any abnormalities, more sensitive imaging techniques should be requested, including bone scan or CT and/or MRI of the femur. Specialist review is recommended.
Management
Once an AFF has been identified, it is recommended that antiresorptive agents, including bisphosphonates and denosumab, be stopped, as ongoing use may delay healing or contribute to a contralateral AFF.4 Further management includes optimisation of vitamin D levels and dietary calcium intake. Patients require multidisciplinary care with an orthopaedic surgeon, an osteoporosis specialist (endocrinologist, geriatrician, rheumatologist) and rehabilitation team in conjunction with their GP.
A patient with a complete AFF will require surgical fixation, preferably with intramedullary rod insertion. However, in the case of an incomplete AFF, patients can either be managed conservatively or with prophylactic surgical fixation. If conservative management is recommended, patients are advised to limit weightbearing on the affected side using a gait aid. Management of incomplete and complete AFFs are shown in the Flowchart.
There is a risk of progression to a complete fracture, with thigh pain and a radiolucent transverse line at the site of cortical beaking being high-risk indicators for progression. Serial radiographs can assist with monitoring for progression of the fracture, which may indicate if prophylactic surgical fixation is required. Early review by an orthopaedic surgeon and osteoporosis specialist is recommended in this instance.
Ongoing management of bone health in patients with AFF is complex and requires specialist assessment. Decision regarding further osteoporosis therapy depends on other clinical factors, including recent fragility fractures and bone density. Further management is made on an individual basis. Patients may be recommended a drug holiday or be prescribed anabolic osteoporosis therapy, such as teriparatide, or other antiresorptive drugs. However, more research is needed to guide the optimal use of osteoporosis therapy following an AFF.
Conclusion
AFFs associated with antiresorptive therapy are rare, but are associated with considerable morbidity and implications for future osteoporosis management. Clinicians need to be aware of AFFs to ensure timely diagnosis, cessation of antiresorptive therapy and referral of the patient to specialist multidisciplinary teams. A patient on antiresorptive treatment who complains of new thigh or hip pain should trigger rigorous radiological assessment to exclude AFFs. Complete AFFs require surgical intervention, whereas patients with incomplete AFFs may be offered prophylactic surgery if pain is present or be managed conservatively. Subsequent management of underlying osteoporosis needs to be considered on an individual basis. ET