Depression or diabetes distress? The importance of screening in adults with type 2 diabetes

Depression
Diabetes type 2
Psychological distress is common in people with type 2 diabetes and is linked with poorer health outcomes. Although depression and diabetes distress are related, they are distinct constructs that differentially impact biological and behavioural diabetes outcomes. Screening for both depression and diabetes distress may help personalise care and inform referral pathways for people with type 2 diabetes.
- Many patients with diabetes experience emotional distress. Although this may mimic depression, it can reflect a patient’s emotional adjustment to a chronic disease.
- Both depressive symptoms and diabetes distress can be assessed using questionnaires such as the Patient Health Questionnaire 9 and the Diabetes Distress Scale.
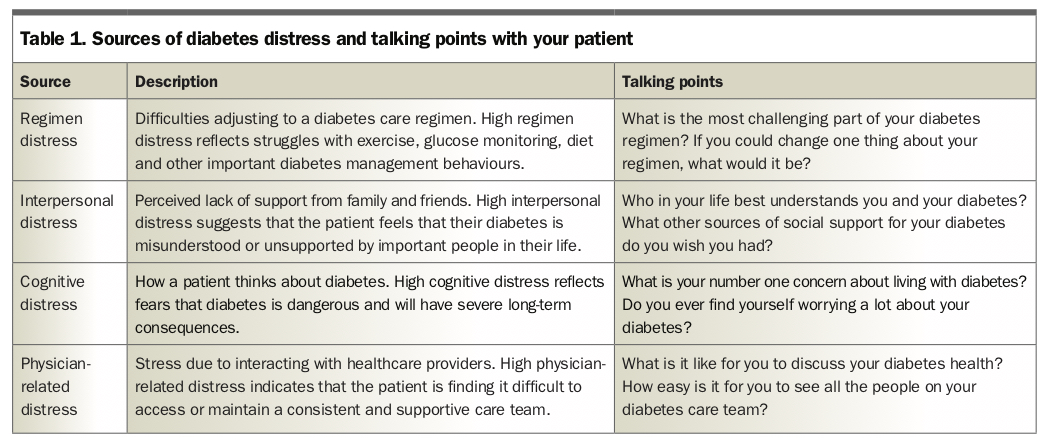
- Diabetes distress comes from four main sources: cognitive distress, interpersonal distress, regimen distress and distress arising from interactions with healthcare providers.
- Individualised treatment is a central principle of type 2 diabetes management and can be optimised by considering a patient’s emotional distress profile in conjunction with their overall treatment goals.
GPs play a central role in diabetes management for the estimated one million adults with type 2 diabetes in Australia.1 Patients with type 2 diabetes experience elevated rates of emotional distress that increase treatment complexity, contribute to greater social and occupational disability, and impact diabetes health and self-management.2 Current general practice management guidelines for type 2 diabetes recommend regular mental health screening to facilitate appropriate intervention and/or referral.3
Questionnaires can provide a brief and effective mental health assessment; however, interpreting these is not always straightforward in the context of type 2 diabetes. For example, symptom scores on common depression inventories can be misleading because some symptoms of depression, such as lethargy or disturbed appetite, are also features of type 2 diabetes.4 Indeed, evidence suggests that large proportions of people with type 2 diabetes who screen positive for depression on questionnaires do not meet criteria for diagnosis of major depressive disorder (MDD) when assessed using a structured clinical interview.5
Some patients with type 2 diabetes who report elevated depressive symptoms may instead be experiencing a form of psychological distress that is specific to diabetes, termed diabetes distress.6,7 Diabetes distress is more common than depression in some people (rates up to 46%), can become chronic, and is more strongly associated with biological (e.g. glycaemic management) and behavioural (e.g. regular exercise) aspects of type 2 diabetes than depressive symptoms.8-10 Screening for both depression and diabetes distress may help GPs distinguish between emotional disturbance reflective of psychiatric illness (e.g. MDD) and distress that occurs as a normative response to managing a chronic and complex illness (i.e. diabetes distress).
Diabetes distress comes from four main sources (Table 1). These are cognitive distress (e.g. fearing long-term health complications), interpersonal distress (e.g. feeling unsupported by family and friends), regimen distress (e.g. coping with a new medical routine), and distress arising from interactions with healthcare providers (e.g. not having a regular GP). Regimen distress has particular relevance to disease management, over and above depressive symptoms.11-13 Patients experiencing severe regimen distress are more likely to experience difficulties with blood glucose management and may benefit most from interventions targeting daily disease management. On the other hand, patients experiencing severe interpersonal distress combined with high levels of depressive symptoms are at risk of more substantial functional impairments and may require more substantial mental health support. By understanding the source(s) of distress, a GP can better select an appropriate care pathway.
{kind=link}
Assessment of depression and diabetes distress
Both depressive symptoms and diabetes distress can be quickly assessed using freely available questionnaires. The Patient Health Questionnaire 9 (PHQ-9) is a brief and useful measure of the severity of symptoms of MDD.14 Total scores on the PHQ-9 of 5 to 9 represent mild depression, 10 to 14 moderate depression, 15 to 19 moderately-to-severe depression and 20 to 27 severe depression. In people with diabetes, a cut-off score of 12 or more is recommended for identifying probable MDD in primary care assessment.15,16
The Diabetes Distress Scale (DDS-17) is a 17-item measure of diabetes-related emotional distress.17 The DDS-17 yields a total score, which is calculated as the average across all items, and also four subscale scores that each address a different kind of distress (i.e. cognitive distress, interpersonal distress, regimen distress and physician-related distress), calculated as mean item scores in each subscale. A score of 3 or more in a subscale indicates clinically relevant distress in that particular subscale.
Choosing a care pathway based on a patient’s distress profile
Individualised treatment is a central principle of type 2 diabetes management and can be optimised by considering a patient’s emotional distress profile in conjunction with their overall treatment goals.18 As already mentioned, regimen and interpersonal distress appear most related to important health outcomes, and therefore being aware of these may help tailor interventions.
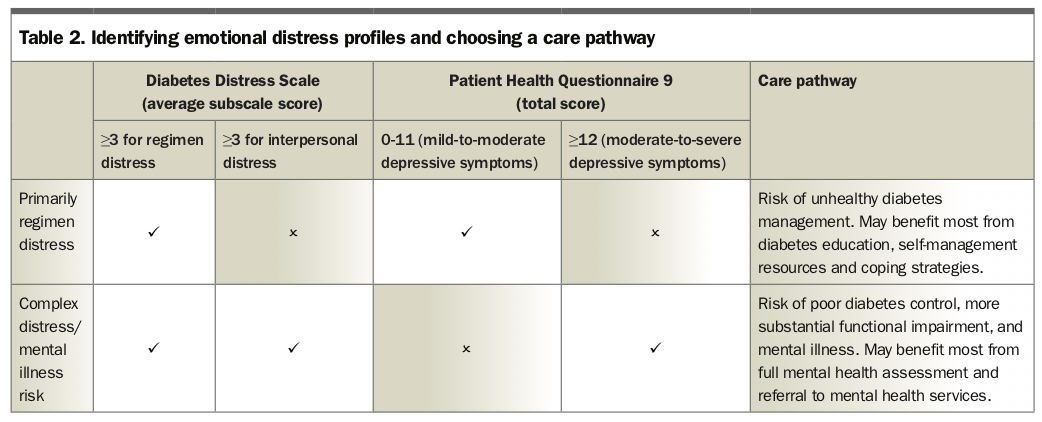
A patient whose distress profile indicates severe regimen distress with mild-depressive symptoms may benefit most from self-care training and collaborative management of regimen demands, rather than interventions that target mood. This may be the most pragmatic way to simultaneously alleviate distress while improving diabetes management. Patients who show a distress profile of moderate-depressive symptoms and broader sources of diabetes distress, especially clinically relevant interpersonal distress, may require more intensive intervention to reduce the impact on general functioning, including face-to-face psychological treatments, online programs for depression in diabetes and/or interpersonal support resources, such as peer-support networks. A decision-making tool for assessing emotional distress profiles is presented in Table 2.
{kind=link}
Discussing diabetes distress with your patient
Many people living with diabetes are sensitive to the potential double stigma of having both a physical and mental health condition.19 Conceptualising diabetes distress as a common aspect of diabetes itself, rather than a psychiatric illness, may further alleviate psychological burden and help the person feel that their condition is manageable.
It may be useful to describe diabetes distress as a well-understood phenomenon and discuss each of the four known sources of diabetes distress with your patient to help understand their key concerns. Talking points to help begin a conversation about the sources of diabetes distress are presented in Table 1. When discussing a patient’s diabetes care it is important to consider the impact that language can have. Diabetes Australia provide a useful guide to supportive language in diabetes care on their website (Box).
{kind=link}
Evidence-based treatments
Although depressive symptoms respond to pharmacotherapy, effects on diabetes health may be limited, and antidepressants that antagonise cholinergic M3-receptors (such as amitriptyline or clomipramine) may be contraindicated in people with diabetes.20-22 Face-to-face cognitive behavioural therapy is effective in reducing depressive symptoms and improving diabetes health.23,24 However, this may not be easily accessible to patients outside metropolitan areas, in which case online therapies may be helpful. For people with mild-to-moderate depressive symptoms, myCompass by Black Dog Institute is freely available and features a diabetes wellbeing module, along with other activities to help manage stress and improve day-to-day functioning. For people with moderate-to-severe depressive symptoms, the depression course available from This Way Up by CRUfAD is effective in addressing both depressive symptoms and some aspects of diabetes distress, although may not improve diabetes health (Box).25
Several approaches to addressing diabetes distress have been trialled and the most effective programs focus on diabetes-specific problem solving and psychological strategies for managing short-term emotional distress.26 If available, a diabetes educator or health psychologist can help the patient identify and address their regimen concerns while building coping skills. Diabetes Australia’s website provides practical suggestions for addressing common difficulties in everyday diabetes management (www.diabetesaustralia.com.au/living-with-diabetes). Online tools, such as myCompass, which offer a broad selection of wellbeing tools, may also help patients manage diabetes distress (Box).
Conclusion
Many patients with diabetes experience emotional distress. Although this may mimic depression on screening questionnaires, it may simply reflect a patient’s emotional adjustment to a chronic disease. Screening for both depression and diabetes can help personalise treatment by understanding a patient’s emotional distress profile. Distress about the demands of a diabetes regimen has a significant impact on diabetes health outcomes, especially glycaemic management. Selecting care pathways that reflect the source of a patient’s emotional distress may lead to better treatment engagement and improved diabetes management. ET
References
2. Nanayakkara N, Pease A, Ranasinha S, et al. Depression and diabetes distress in adults with type 2 diabetes: results from the Australian National Diabetes Audit (ANDA) 2016. Sci Reports 2018; 8: 7846.
5. Fisher L, Skaff MM, Mullan JT, et al. Clinical depression versus distress among patients with type 2 diabetes not just a question of semantics. Diabetes Care 2007; 30: 542-548.
6. Dieter T, Lauerer J. Depression or diabetes distress? Perspect Psychiatr Care 2018; 54: 84-87.
7. Beeney L. Identifying and managing diabetes distress: not mad, more likely sad. Endocrinol Today 2015; 4(2): 21-23.
8. Fisher L, Polonsky WH, Hessler DM, et al. Understanding the sources of diabetes distress in adults with type 1 diabetes. J Diabetes Complicat 2015; 29: 572-577.
10. Fisher L, Hessler D, Glasgow RE, et al. REDEEM: a pragmatic trial to reduce diabetes distress. Diabetes Care 2013; 36: 2551-2558.
11. Hessler D, Fisher L, Strycker LA, Arean PA, Bowyer V. Causal and bidirectional linkages over time between depression and diabetes regimen distress in adults with type 2 diabetes. Diabetes Res Clin Pr 2015; 108: 360-366.
12. Hessler D, Fisher L, Glasgow RE, et al. Reductions in regimen distress are associated with improved management and glycemic control over time. Diabetes Care 2014; 37: 617-624.
13. Martinez K, Lockhart S, Davies M, Lindsay JR, Dempster M. Diabetes distress, illness perceptions and glycaemic control in adults with type 2 diabetes. Psychol Health Med 2018; 23: 171-177.
19. Clarke J, Proudfoot J, Vatiliotis V, et al. Attitudes towards mental health, mental health research and digital interventions by young adults with type 1 diabetes: a qualitative analysis. Health Expect 2018; 21: 668-677.
20. Semenkovich K, Brown ME, Svrakic DM, Lustman PJ. Depression in type 2 diabetes mellitus: prevalence, impact, and treatment. Drugs 2015; 75: 577-587.
21. Salvi V, Grua I, Cerveri G, Mencacci C, Barone-Adesi F. The risk of new-onset diabetes in antidepressant users – a systematic review and meta-analysis. PLos One 2017; 12: e0182088.
22. Tran Y-H, Schuiling-Veninga CC, Bergman JE, Groen H, Wilffert B. Impact of muscarinic m3 receptor antagonism on the risk of type 2 diabetes in antidepressant-treated patients: a case-controlled study. CNS Drugs 2017; 31: 483-493.
23. Li C, Xu D, Hu M, et al. A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for patients with diabetes and depression. J Psychosom Res 2017; 95: 44-54.
24. Safren SA, Gonzalez JS, Wexler DJ, et al. A randomized controlled trial of cognitive behavioral therapy for adherence and depression (CBT-AD) in patients with uncontrolled type 2 diabetes. Diabetes Care 2014; 37: 625-633.
25. Newby J, Robins L, Wilhelm K, et al. Web-based cognitive behavior therapy for depression in people with diabetes mellitus: a randomized controlled trial. J Med Internet Res 2017; 19: e157.
26. Schmidt C, Loon PB, Vergouwen A, Snoek F, Honig A. Systematic review and meta-analysis of psychological interventions in people with diabetes and elevated diabetes distress. Diabetic Med 2018; 35: 1157-1172.