Preventing the fracture cascade

Fractures
Osteoporosis
People who experience a minimal trauma (or osteoporotic) fracture are at least twice as likely to sustain further fractures, with significant associated morbidity and mortality. There are a range of safe and effective nonpharmacological and pharmacological strategies to reduce the risk of recurrent fracture. Therefore, patients with an incident osteoporotic fracture should be identified and treated early to prevent the fracture cascade.
- A minimal trauma fracture at any site increases the risk of sustaining further fractures by at least twofold, whereas vertebral and hip fractures increase the risk by at least fourfold.
- Minimal trauma fractures are associated with significant morbidity and premature mortality.
- Both nonpharmacological and pharmacological strategies can be used to manage osteoporosis and fracture risk, and interventions should be tailored to the patient’s risk level, preference, compliance, comorbidities and medication side effects.
- Denosumab and bisphosphonates are both excellent pharmacological options for patients at high risk of osteoporotic fracture.
- The duration of pharmacotherapy should be determined by balancing the risk of further fracture with the risk of short-term and long-term medication side effects.
Picture credit: © Judith/adobe.com
Osteoporosis is a disorder involving microarchitectural deterioration of bone and low bone mass, resulting in reduced bone strength, which leads to fractures that occur with minimal trauma (i.e. an impact equivalent to a fall from standing height or lower).1 In 2012, a reported 140,822 minimal trauma fractures (MTFs) occurred in Australia; by 2022, this figure is expected to increase to 183,105.2 More than 50% of postmenopausal women and 30% of men over the age of 60 years will experience at least one osteoporotic fracture during their remaining lifetime,3 with nonhip, nonvertebral fractures accounting for 80% of all incident fractures in people aged 50 to 69 years.2
An MTF confers a high risk of morbidity and mortality, from both the fracture itself and further fractures. People who have had an MTF are at least twice as likely to sustain further fractures, especially within the first two years after the initial fracture.4,5 Those with vertebral and hip fractures have at least a fourfold increased risk of further fracture.6-8 Although men sustain fewer initial fractures than women, men are more likely to refracture and have higher mortality after an initial fracture.5,9 Moreover, excess mortality occurs after all proximal osteoporotic fractures, particularly in the first five years, and this risk may persist for up to 10 years after a hip fracture. A substantial proportion of the increased mortality risk is associated with recurrent fracture.9
Osteoporosis pharmacotherapy is safe and can reduce the risk of refracture by up to 70%, but the fear of uncommon treatment-related complications has led to uncertainty about the duration of therapy. Fewer than 20% of patients are appropriately assessed and treated for the underlying cause of an MTF (i.e. osteoporosis).10 Thus, it is imperative to identify patients who have sustained an MTF and to treat them early to reduce the risk of refracture, thereby preventing the fracture cascade. This article uses a case study and draws from the 2017 Royal Australian College of General Practitioners guidelines for osteoporosis management11 to detail the practical aspects of secondary fracture prevention.
Risk factor assessment
Jill is a 64-year-old woman who has sustained a wrist fracture after tripping on an uneven footpath. She has a background of chronic obstructive pulmonary disease (COPD), hypertension and type 2 diabetes. How would you assess the clinical risk factors for Jill’s MTF?
A clinical osteoporosis risk factor assessment should be undertaken for every patient who sustains an MTF. This initially involves a thorough history and examination. There are a range of clinical risk factors for osteoporotic fracture (Box), but some of the most important are prior MTF, recurrent falls, older age and female sex. Specific enquiry should be made regarding height loss (of more than 2.5 cm), long-term corticosteroid use, gluten intolerance, malabsorptive symptoms, family history of osteoporosis (parental history of hip fracture) and history of hyperthyroidism. In women, menarche, age at menopause and history of oligomenorrhoea should be elicited, together with prior use of hormone replacement therapy (HRT). In men, symptoms of hypogonadism, including reduction in libido and shaving frequency, should be ascertained. Lifestyle factors including smoking, alcohol consumption, dietary calcium intake, sunlight exposure and exercise should be ascertained.
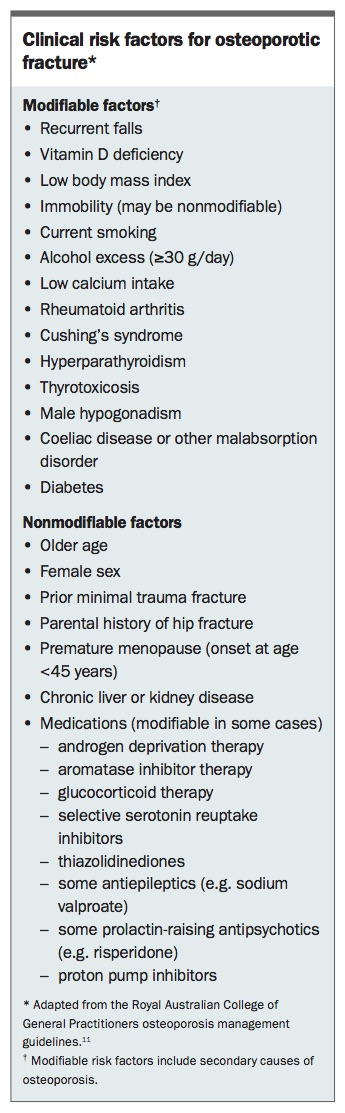{kind=link}
On examination, evidence of thoracic kyphosis and focal bony tenderness can indicate vertebral fractures. An increased wall-to-occiput distance (greater than 0 cm) may be a sign of vertebral fracture. The examination should include checking for signs of thyrotoxicosis (e.g. tachycardia, sweats) and Cushing’s syndrome (e.g. hypertension, facial plethora, abdominal striae, proximal muscle weakness, bruising). Baseline weight and height are simple measures to monitor; height loss is a potential indicator of further vertebral fractures, and significant weight loss is often accompanied by a reduction in bone mineral density (BMD).
Investigations
On further enquiry, you establish that Jill’s COPD has been managed with two-week courses of corticosteroids about three times a year. She underwent menopause at 43 years of age but did not take HRT. Her diabetes is well controlled (HbA1c of 6.9%) with metformin and she has no history of hypoglycaemia. On examination, she is normotensive with no postural hypotension. She does not have a Cushingoid appearance. She has mild thoracic kyphosis but no focal tenderness. What further investigations would you perform?
Dual-energy x-ray absorptiometry (DXA) is the gold-standard investigation to determine BMD and forms an important component of fracture risk assessment. DXA is noninvasive, simple and involves exposure to low levels of radiation (equivalent to a return trans-Atlantic flight or one-sixth of the exposure from a chest x-ray).12,13 Thus, it is used for initial assessment of osteoporosis and long-term monitoring. Table 1 defines BMD diagnostic criteria using DXA. Notably, about half of all first MTFs occur in people with T-scores in the osteopenic range (T-score between –1 and –2.5 SD).14 Moreover, a normal BMD does not exclude the diagnosis of osteoporosis; a person who has had an MTF but has normal BMD on DXA can still have osteoporosis. Secondary causes of osteoporosis should be considered in all patients, particularly those with multiple fractures or a Z-score (the age- and sex-matched BMD measurement) of –2.0 or less.
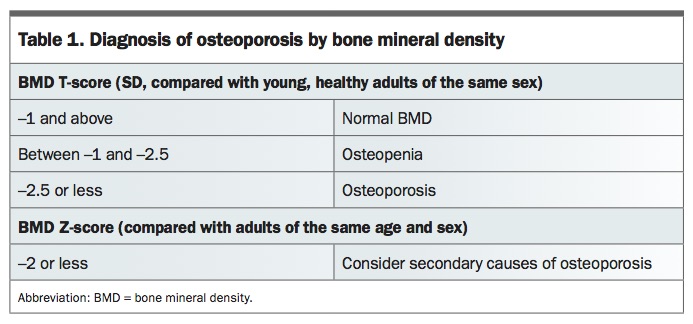{kind=link}
As osteoarthritis may cause lumbar spine BMD to be falsely elevated on DXA, assessment of BMD using quantitative computed tomography may be considered if hip BMD is not measurable (because of bilateral hip replacements) or is in the normal range. However, it is not used as a first-line investigation because it is associated with radiation exposure more than 20 times higher than that from DXA and there are limited data regarding its effectiveness for fracture prediction compared with DXA.
Additional suggested investigations for Jill include assessment of baseline renal function (to guide treatment choice) and measurement of serum calcium (for hypercalcaemia or hypocalcaemia), phosphate (hypophosphataemia), vitamin D and thyroid- stimulating hormone (hyperthyroidism) levels. Other investigations to determine secondary causes of osteoporosis include screening tests for coeliac disease and myeloma. A thoracolumbar spine x-ray is needed to look for prevalent vertebral fractures, which would have significant implications for future fracture risk. A vertebral fracture assessment, wherein thoracic and lumbar spine images are obtained during DXA, can also be performed as a screening test; however, there is no Medicare rebate for this service.
Management
Preventing further fractures
Jill’s bone densitometry test results show a T-score of –2.0 SD at the lumbar spine and –2.1 SD at the femoral neck. The corresponding Z-scores are –1.9 SD and –1.7 SD. Her pathology test results show normal renal function and normal levels of calcium, phosphate and thyroid-stimulating hormone. Her 25-hydroxyvitamin D level is 35 nmol/L. Results of her screening tests for coeliac disease and myeloma are negative. How would you reduce her risk of further fractures?
With recent nonvertebral fracture, osteopenia and premature menopause, Jill is at high risk of further osteoporotic fracture and would benefit from antiresorptive therapy. Patients with hip or vertebral fractures are also at high risk of future fracture and would benefit from osteoporosis pharmacotherapy independent of the DXA result. However, if there is uncertainty about fracture risk, an online absolute fracture risk calculator (e.g. Fracture Risk Assessment Tool [www.shef.ac.uk/FRAX] or Garvan Fracture Risk Calculator [https://www.garvan.org.au/bone-fracture-risk]) may be a useful tool to guide therapy and for patient education.11
There are a range of nonpharmacological and pharmacological measures that could be used to reduce Jill’s risk of further fractures. Australian guidelines recommend several nonpharmacological strategies for patients with osteoporosis, including multifactorial falls prevention strategies, weightbearing exercises and optimising vitamin D and calcium intake (Table 2).11,15-23 In addition to antiresorptive therapy, Jill should be encouraged to optimise weightbearing exercise and employ strategies to avoid falling, such as exercising to improve muscle strength and balance and reviewing environmental hazards and risks from medications. Adequate vitamin D and calcium intake are important to prevent adverse effects from pharmacotherapy, and there is evidence of small reductions in fracture risk.21,22 Calcium supplementation has also been an area of controversy, with conflicting data regarding its effect on cardiovascular risk.24 However, if adequate calcium intake cannot be maintained through diet alone,25 supplementation up to the recommended levels shown in Table 2 is appropriate.
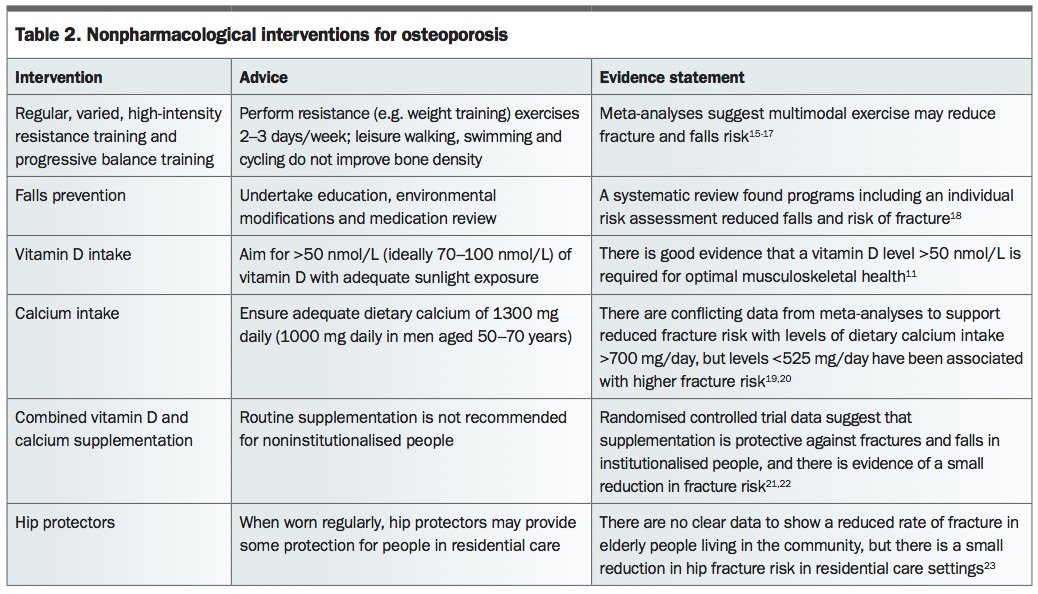{kind=link}
Pharmacotherapy
Jill has osteoporosis with a recent MTF despite having a BMD in the osteopenic range. Given that Jill would benefit from antiresorptive therapy in addition to nonpharmacological measures, what pharmacological approach would you take to manage her future risk of fractures?
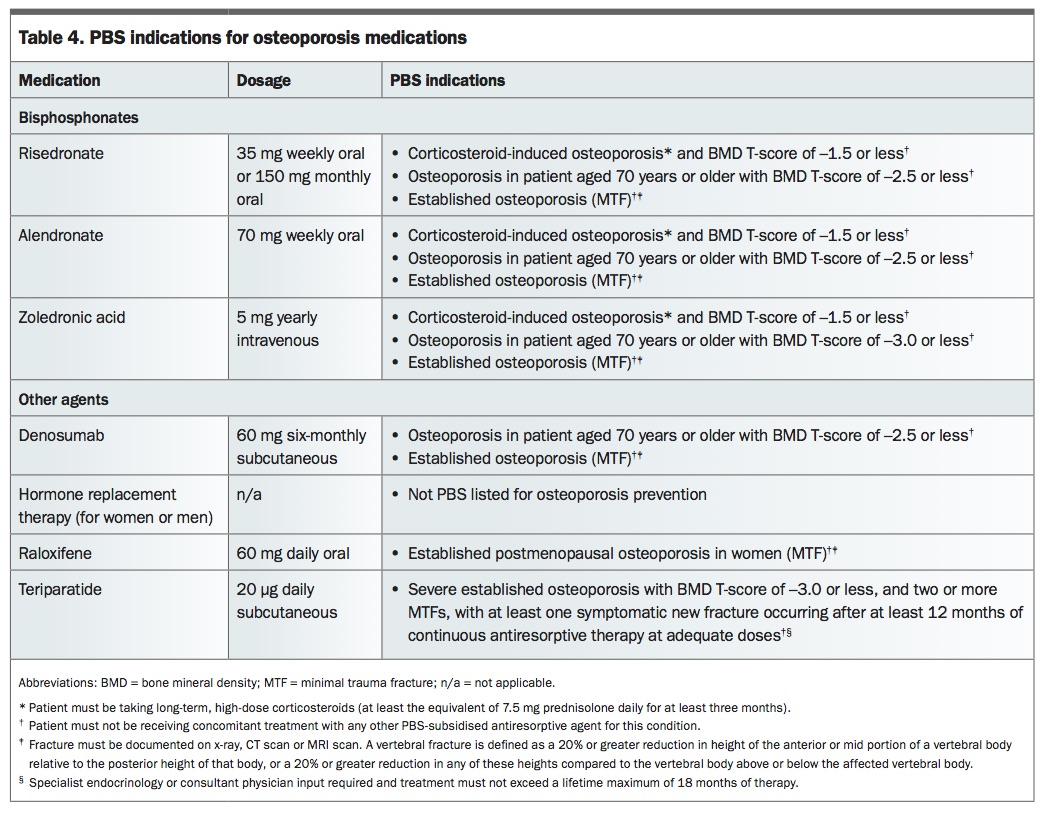
The choice of pharmacotherapy should be determined based on a patient’s comorbidities, likely compliance and preference, and medication side effects. Medications for the treatment of osteoporosis, along with their antifracture efficacy and side effects, are shown in Table 3;26-35 the PBS indications for each are shown in Table 4.
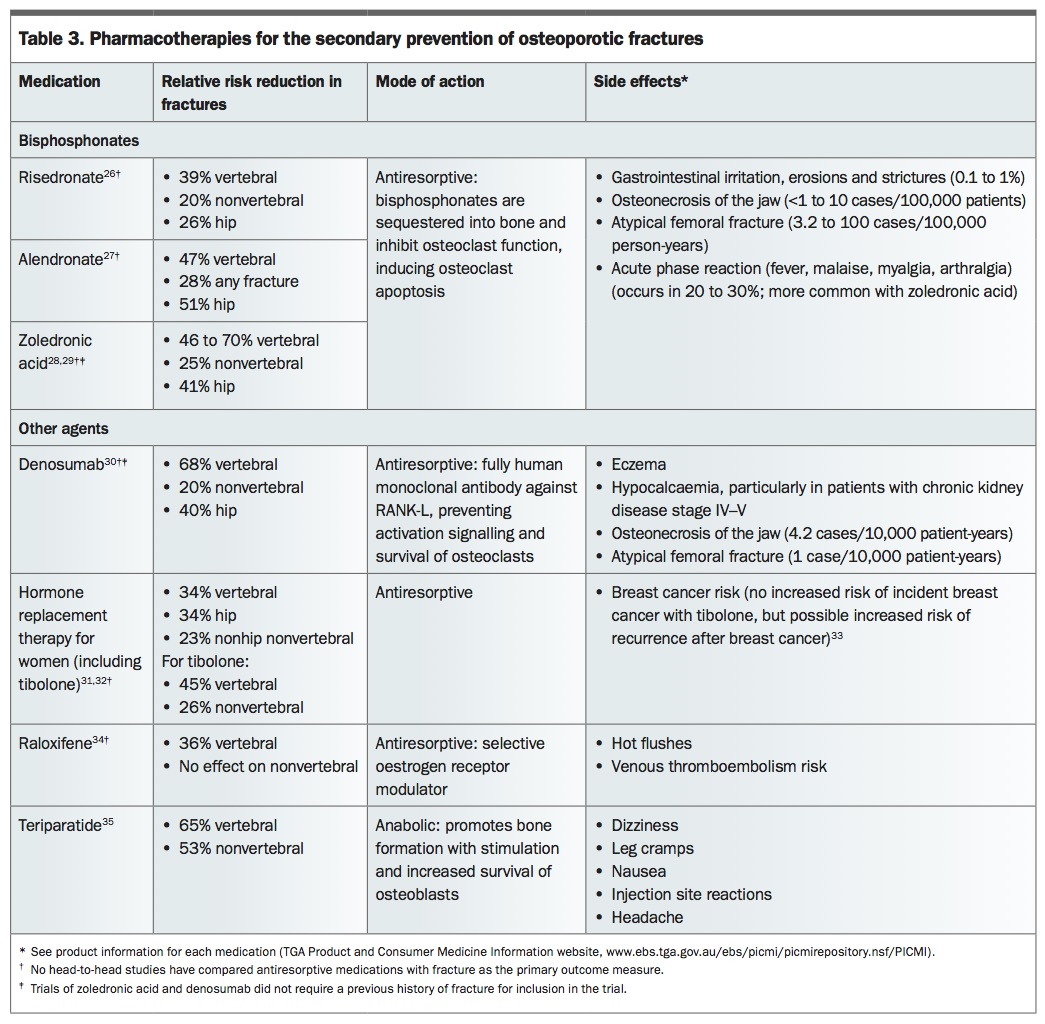{kind=link}
{kind=link}
Bisphosphonates and denosumab
Antiresorptive agents in the form of bisphosphonates and denosumab are first-line agents for treatment of men and postmenopausal women with osteoporosis. Bisphosphonates are first-line agents for patients with corticosteroid-induced osteoporosis. These antiresorptive medications are subsidised by the PBS for any patient with an MTF, irrespective of BMD T-score (Table 4), but it is up to the treating physician to balance the benefits and risks of starting therapy in each patient.
Oral bisphosphonates, intravenous bisphosphonates (zoledronic acid) and denosumab have similar antifracture efficacy, but each has unique limitations that need to be considered before starting therapy (Table 3). Oral bisphosphonates are associated with gastritis and oesophagitis with long-term use.36 Moreover, they require specific administration instructions (remaining upright for 30 minutes after ingestion) and, similar to many oral medications, have poor patient compliance after one year.37 Enteric-coated formulations of oral bisphosphonates can be taken with food, which may help with compliance, but patients must still remain upright for 30 minutes afterwards. On the other hand, compliance is ensured with yearly intravenous infusions of zoledronic acid or six-monthly subcutaneous injection of denosumab.
The most common adverse effect with zoledronic acid is an influenza-like or acute phase reaction, which occurs in about 30% of patients after the first infusion, although its severity diminishes with subsequent infusions. Bisphosphonates should not be used if creatinine clearance is less than 35 mL/min, and zoledronic acid should be dose-reduced if creatinine clearance is less than 60 mL/min. Denosumab has a slightly higher risk of eczema (3.1% vs 1.7% for placebo)38 but is otherwise well tolerated. Although denosumab is not renally cleared (in contrast to bisphosphonates) and can be used in patients with chronic kidney disease, caution should be exercised when the creatinine clearance is less than 30 mL/min, because of an increased risk of hypocalcaemia irrespective of calcium and vitamin D intake. Moreover, as chronic kidney disease affects bone health in different ways, specialist input should be sought for such patients.
Omitting or delaying a dose of denosumab results in rapid rebound bone loss in the next six to 12 months; there have been case reports of vertebral fractures occurring after denosumab cessation.39 It is therefore crucial to adhere to the six-monthly regimen of denosumab. Bisphosphonates, on the other hand, have not been associated with rebound fractures. Overall, denosumab and bisphosphonates are both excellent options for patients at high risk of osteoporotic fracture. To reduce the risk of hypocalcaemia, it is important to ensure the patient’s vitamin D level is greater than 50 nmol/L before starting therapy, even in patients with normal renal function.
Other antiresorptive and anabolic agents
Selective oestrogen receptor modulators, such as raloxifene, have oestrogen agonist activity on the bone and antagonist activity at the breast, with data indicating they reduce invasive breast cancer recurrence.40 These agents can be considered for younger postmenopausal women (aged in their 50s or early 60s) with primarily vertebral osteoporosis, as they have been shown to reduce the risk of vertebral fractures only.41 HRT may also be considered for younger postmenopausal women at moderate to high risk of fracture and with menopausal symptoms. In a subanalysis of the Women’s Health Initiative study, adverse effects of HRT, including risk of stroke and breast cancer, increased only after 60 years of age.42 Therefore, the use of HRT up to 60 years of age is a reasonable option for a woman aged in her 50s who has osteoporosis and hot flushes.
Teriparatide is a parathyroid hormone analogue and the only anabolic agent available in Australia on the PBS, which limits its use to patients with severe osteoporosis and requires that it be initiated by a specialist (Table 4). It is contraindicated in patients at high risk of osteosarcoma, including those with Paget’s disease, bone metastases or previous radiotherapy. However, registry studies have shown that osteosarcoma has not been increased in people treated with teriparatide.43
Recurrent fractures
Investigations
Jill starts taking an oral bisphosphonate, alendronate 70 mg weekly, and continues taking this for five years. She returns aged 69 years with back pain and is found to have a fractured L1 vertebral body (Figure 1). What should be done next?
{kind=link}
When a patient has a recurrent fracture while taking pharmacotherapy, reassessment of risk factors, review of patient compliance and exclusion of secondary causes, as guided by the clinical history and examination, should occur.
Management
Jill has no clinical features or results of investigations that suggest a secondary cause. However, she reports taking the alendronate 30 minutes after breakfast. A DXA scan gives a T-score of –3.1 SD at the lumbar spine (i.e. a decline of 10% over five years). What changes could be instituted in Jill’s management?
Jill has sustained a further fracture and had a decline in BMD while taking antiresorptive therapy; however, she has been using an incorrect administration technique for the medication. Parenteral therapy, in the form of yearly zoledronic acid infusions or six-monthly subcutaneous denosumab injections, should therefore be considered. As Jill may meet the PBS indications for teriparatide (although she has effectively not had adequate bisphosphonate absorption, if any at all), this could also be an appropriate option, and may offer greater fracture reduction over the bisphosphonates.44
Duration of pharmacotherapy
Jill elects to undergo annual zoledronic acid infusions, which she tolerates well. Three years later, at the age of 72 years, her BMD is stable and she has remained fracture-free. How long would you continue her bisphosphonate therapy?
Guidelines recommend continuing bisphosphonate therapy in patients who are at high risk of recurrent fracture, especially those with a T-score at the femoral neck of –2.5 SD or lower at the time of reassessment or with previous hip or vertebral fractures.11 Cessation of denosumab is not advised because of its rapid reduction in action after six months.
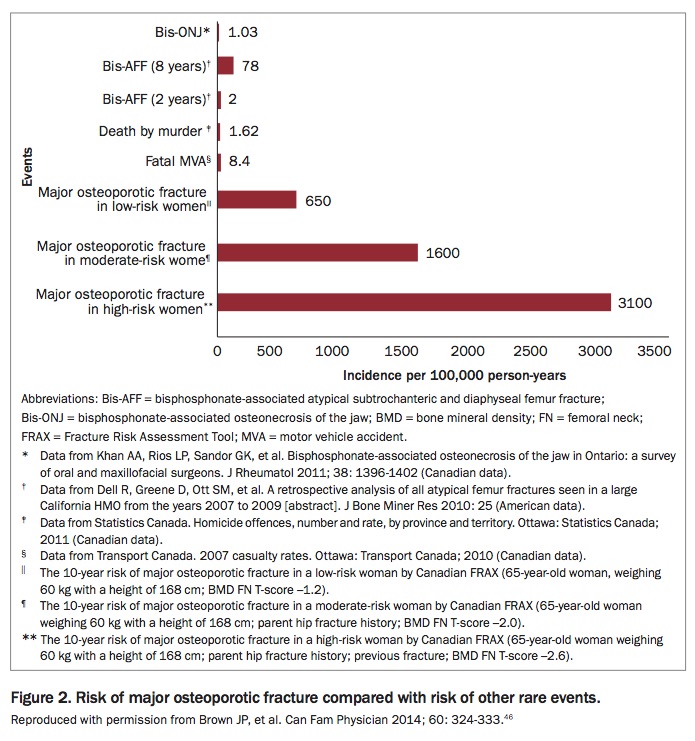
Although long-term use of bisphosphonates may be associated with higher risk of osteonecrosis of the jaw and atypical femoral fracture (up to 100 cases per 100,000 person-years for the latter), this risk is much lower than the risk of recurrent osteoporotic fracture.45 In making treatment decisions, the very low risk of these events must be weighed against the significant benefits of treatment in preventing osteoporotic fractures (Figure 2).46 Long-term outcome studies suggest that osteoporosis treatments are safe and have demonstrated long-term antifracture efficacy.47,48 Overall, there is no defined duration for which antiresorptive therapy should continue, but in people who are at very high risk of recurrent fracture, treatment may continue beyond 10 years.
{kind=link}
As Jill is at high risk of future fracture in the context of a prior vertebral fracture, she should continue with bisphosphonate therapy for at least another two years. Jill’s fracture risk should be reassessed in about two years to help determine the duration of therapy, but it can be extended to beyond five years.
Conclusion
Sustaining one MTF signifies an increased risk of further fracture, with each successive fracture associated with increasing mortality risk. Clinical risk factor assessment should be undertaken in all patients who sustain an MTF. Appropriate investigations, including a DXA scan, may help stratify those who require treatment. Treatment decisions should be guided by the risk of refracture, the patient’s comorbidities, likely compliance and preference and medication side effects. It is crucial that people who sustain an MTF undergo appropriate investigation and treatment, to prevent the fracture cascade. ET
References
3609-3617.