Glucagon-like peptide-1 receptor agonists – practical use in type 2 diabetes

Diabetes type 2
Diabetes medicines
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are being increasingly prescribed for people with type 2 diabetes. They have been practice-changing owing to their glycaemic, cardiovascular, renal and weight loss benefits, and decreases in all-cause mortality. However, counselling is crucial to advise patients of safe injection techniques and common adverse events such as nausea, which may lead to cessation and avoidance of this therapeutic class. A four-phase approach to selecting, counselling and following up patients can help GPs to prescribe GLP-1RAs safely and effectively.
- Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have multiple glycaemic and nonglycaemic benefits in patients with type 2 diabetes, including reduced glycaemia, mortality, cardiovascular events and weight.
- GLP-1RAs should be considered as second-line therapy in people with type 2 diabetes, especially those with established atherosclerotic cardiovascular disease.
- Effective counselling on injection technique, dose titration and adverse effects can improve adherence to this therapeutic class.
- Prompt follow up can identify adverse effects early and enable decisive management.
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are an increasingly prescribed class of antihyperglycaemic agents for people with type 2 diabetes owing to their glycaemic efficacy with a low risk of hypoglycaemia (except when used in combination with insulin or a sulfonylurea) and proven cardiovascular, renal and weight loss benefits.1,2 GLP-1RAs have been available on the PBS since 2010.3 There are currently three PBS-subsidised GLP-1RAs – dulaglutide, exenatide and semaglutide – with different administration frequencies and devices. A discussion about the non-PBS subsidised GLP-1RA agents, such as liraglutide, is beyond the scope of this article. This article presents a four-phase approach to selecting, counselling and following up patients to help GPs in prescribing GLP-1RAs safely and effectively (see Box 1).
{kind=link}
Mechanism of action of GLP-1RAs
Glucagon-like peptide-1 is a peptide hormone that increases insulin secretion and decreases glucagon secretion from the pancreas in a glucose-dependent manner.4 GLP-1RAs act as agonists at glucagon-like peptide-1 receptors in the gut and brain, delaying gastric emptying and increasing satiety. Overall, the net effects include reduced calorie intake, weight and glucose levels, and increased insulin sensitivity.4 Although dipeptidyl peptidase-4 (DPP-4) inhibitors increase glucagon-like peptide-1 levels, the elevation is small compared with administration of GLP-1RAs.5
Phase 1. Considering prescribing
Current prescribing guidelines from the Australian Diabetes Society recommend GLP-1RAs as next-line therapy in patients who have failed to meet their glycaemic target with usual first-line therapy of metformin and as the first injectable medication before the addition of insulin.2,6 The Australian evidence-based clinical guidelines for diabetes recommend GLP-1RAs as an add-on therapy in patients with cardiovascular disease, multiple cardiovascular risk factors or kidney disease, and intolerance or a contraindication to sodium-glucose cotransporter 2 (SGLT-2) inhibitors.7 Similarly, a joint guideline by the American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD) recommends GLP-1RAs as second- or third-line therapy in patients with predominantly atherosclerotic cardiovascular disease, a compelling need to minimise hypoglycaemia or a need to promote weight loss.1 GLP-1RAs can be added to any combination of other therapies (except DPP-4 inhibitors), including insulin and SGLT-2 inhibitors, although this is not subsidised by the PBS.6
Expected benefits of GLP-1RAs
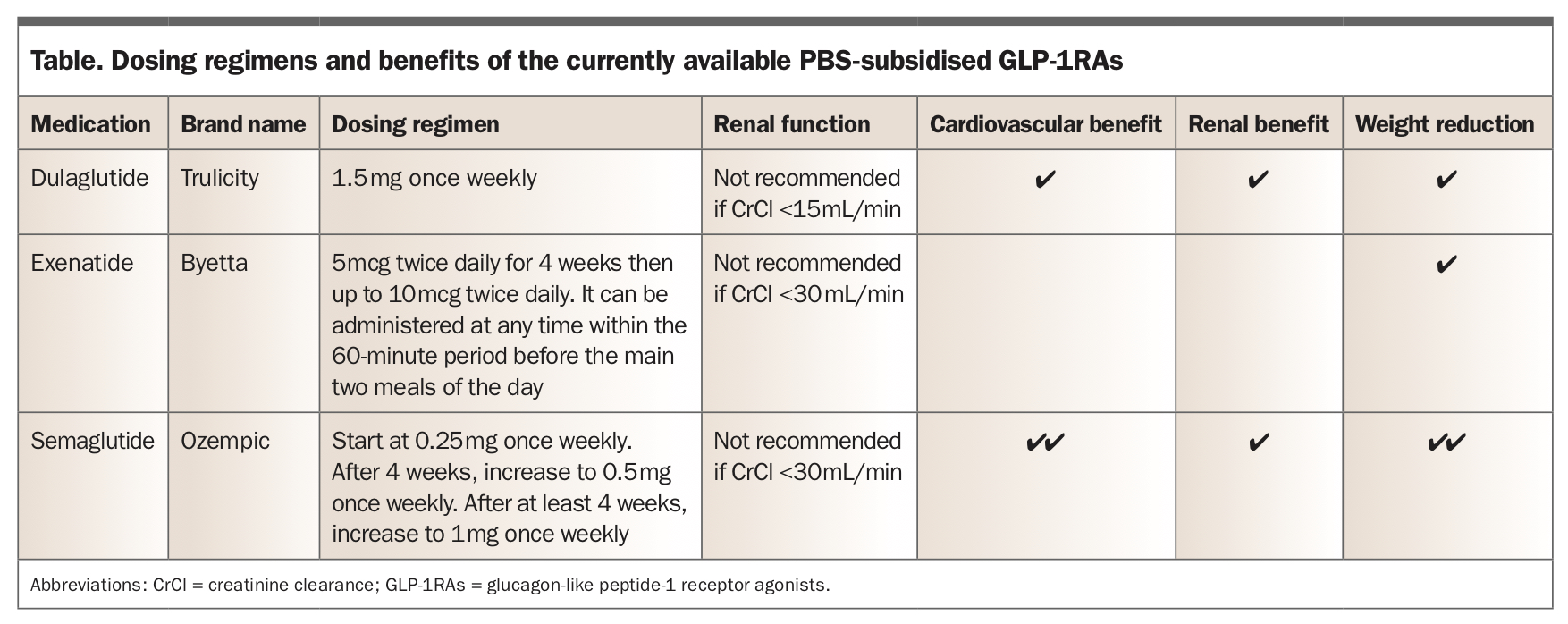
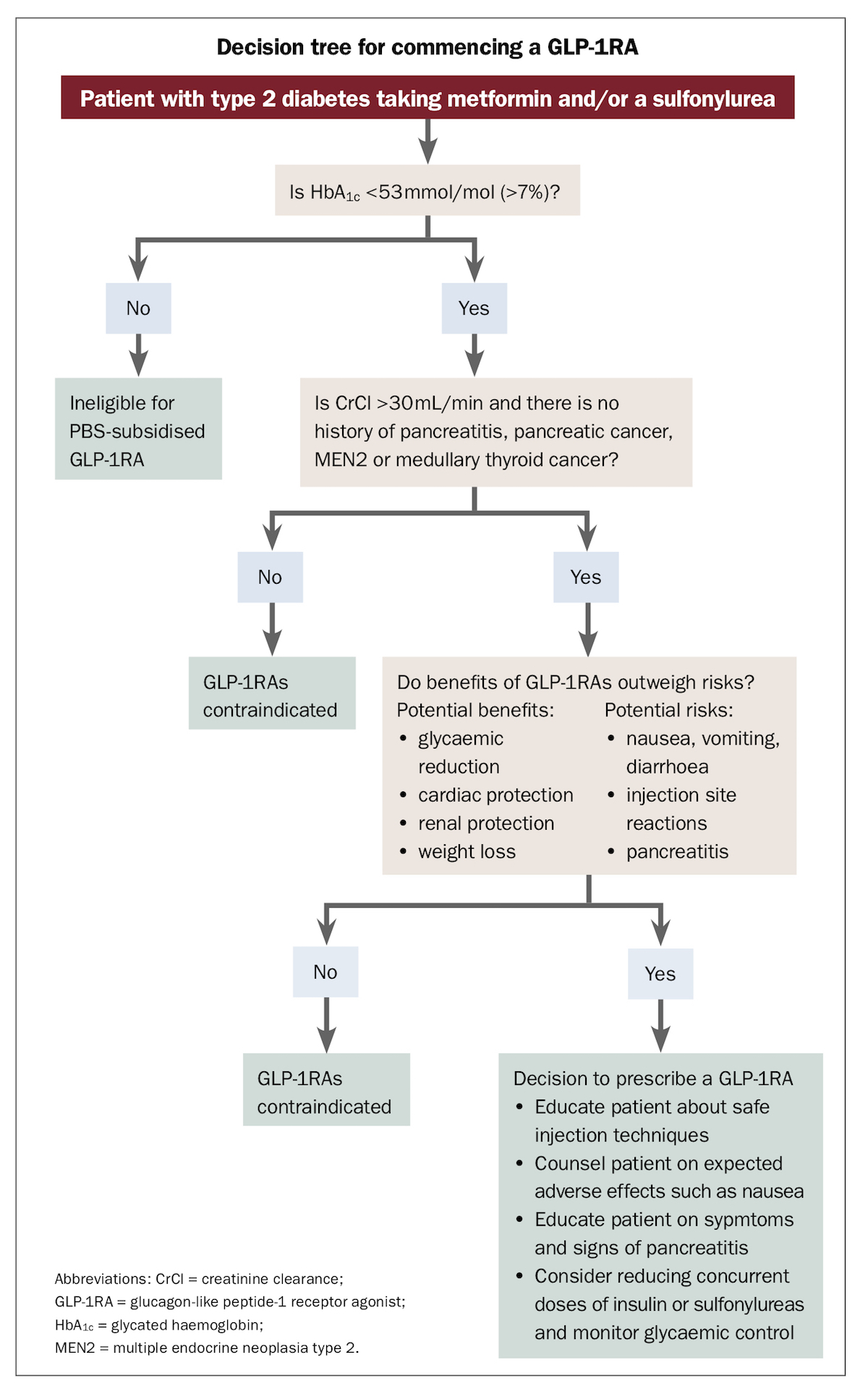
Benefits of the currently available PBS-subsidised GLP-1RAs are summarised in the Table. A decision tree for commencing a GLP-1RA is also shown in the Flowchart.
{kind=link}
{kind=link}
Glycaemic efficacy
GLP-1RAs are one of the most potent antihyperglycaemic classes, with subcutaneous semaglutide exerting the greatest effects on glycated haemoglobin (HbA1c), with a difference compared with placebo of −1.33 percentage points (95% confidence interval [CI] −1.50 to −1.16 percentage points), followed by dulaglutide and exenatide in a descending order of potency.8 Weekly doses of GLP-1RAs preferentially improve fasting blood glucose levels, whereas daily or twice daily doses improve postprandial blood glucose levels to a greater degree.9
All-cause mortality reduction
In a systematic review and meta-analysis of cardiovascular outcome trials (ELIXA, LEADER, SUSTAIN-6, EXSCEL, Harmony Outcomes, REWIND, PIONEER 6), use of GLP-1RAs reduced all-cause mortality by 12% compared with placebo (hazard ratio [HR] 0.88; 95% CI 0.83 to 0.95).10 Similarly, another systematic review and meta-analysis of 764 randomised controlled trials also showed a reduction in all-cause mortality with use of GLP-1RAs (odds ratio [OR] 0.88; 95% CI 0.83 to 0.94).11
Cardiovascular risk reduction
In a systematic review and meta-analysis of cardiovascular outcome trials, use of GLP-1RAs reduced major adverse cardiac events (HR 0.88; 95% CI 0.82 to 0.94, p<0.001) and cardiovascular mortality (HR 0.88; 95% CI 0.81 to 0.96).10 In particular, cardiovascular benefits were greatest with subcutaneous semaglutide, followed by dulaglutide.12 The use of GLP-1RAs reduced the risk of hospital admission for heart failure (HR 0.91; 95% CI 0.83 to 0.99), although to a lesser degree than SGLT-2 inhibitors.10
Renal protection
GLP-1RAs, particularly dulaglutide and semaglutide, may be beneficial for renal protection largely by reducing proteinuria.10,13 In contrast to SGLT-2 inhibitors, GLP-1RAs do not significantly prevent decreases in estimated glomerular filtration rate or increases in creatinine levels.14,15 We await outcomes of the FLOW study, which is dedicated to assessing the renal benefits of semaglutide.
Weight reduction
Compared with placebo, use of dulaglutide 1.5 mg once weekly led to a 1.5 kg (95% CI 1.3 to 1.7 kg) weight reduction over five years.16 Exenatide 5 mcg twice daily (mean ± standard deviation; −2.8 ± 0.3 kg) and 10 mcg twice daily (−3.1 ± 0.3 kg) also led to a greater weight reduction than placebo (−1.4 ± 0.3 kg) at 24 weeks.17 The greatest weight loss was achieved with the use of semaglutide. A dose of 1.0 mg once weekly of semaglutide (maximum dose subsidised by the PBS) achieved a weight reduction of 4.3 kg compared with placebo over two years.18 An even greater weight reduction of 9.6% was achieved with a higher dose of 2.4 mg weekly over 68 weeks in a trial in adults with overweight or obesity and diabetes.19
Comparison with SGLT-2 inhibitors
Both GLP-1RAs and SGLT-2 inhibitors reduce all-cause and cardiovascular mortality.11 As per the ADA and EASD guidelines, the choice of add-on therapy if patients have cardiovascular disease should be either a GLP-1RA or SGLT-2 inhibitor.1 Compared with SGLT-2 inhibitors, GLP-1RAs demonstrate a greater reduction in HbA1c and weight loss.20 However, GLP-1RAs have less profound effects on reduction of hospitalisations for heart failure and renal protection than SGLT-2 inhibitors.14
Recommendations
The results above have prompted the ADA and EASD to recommend GLP-1RAs as preferred second- or third-line injectable agents following metformin in people with:1
- established atherosclerotic cardiovascular disease
- a need to minimise weight gain or promote weight loss
- a need to minimise hypoglycaemia
- mild-to-moderate chronic kidney disease.
Contraindications to GLP-1RAs
There is mixed evidence regarding adverse effects of GLP-1RAs, such as pancreatitis, pancreatic cancer, retinopathy and medullary thyroid cancer. Incidences of acute pancreatitis and pancreatic cancer were reported to be increased with use of GLP-1RAs in the US Food and Drug Administration’s database studies.21,22 However, no association was found between pancreatitis and use of GLP-1RAs in the randomised controlled cardiovascular outcome trials, meta-analyses and systematic reviews.10,23,24 Similarly, there was no increased risk of pancreatic cancer associated with GLP-1RAs in a large cohort study and a 2020 meta-analysis.25,26
There was no significant difference in diabetic retinopathy between placebo and GLP-1RAs, except for an increased risk with subcutaneous semaglutide (OR 1.75; 95% CI 1.10 to 2.78) in the SUSTAIN-6 trial.8 It is unclear whether this retinopathy is a true adverse effect related to a molecule-specific effect of semaglutide or whether it relates to rapid marked reduction in glucose, such as originally described in the Diabetes Control and Complications Trial.27 While we await outcomes of the FOCUS trial, which is dedicated to assessing the effects of semaglutide on eye health, patients using subcutaneous semaglutide should be counselled about the increased risk of retinopathy.
A higher incidence of thyroid C-cell adenomas and carcinoma with use of extended-release exenatide has been seen in rodent studies.28 In the EXSCEL trial in humans, medullary thyroid carcinomas were found in two patients in the exenatide group compared with one patient in the placebo group; however, these individuals all had elevated calcitonin levels at baseline.29
Given the above admittedly inconsistent evidence, contraindications for the use of GLP-1 RAs are:
- a history of pancreatitis
- pancreatic cancer
- multiple endocrine neoplasia type 2
- medullary thyroid carcinoma
- creatinine clearance less than 30 mL/min for exenatide and semaglutide
- creatinine clearance less than 15 mL/min for dulaglutide.
Phase 2. Initial counselling
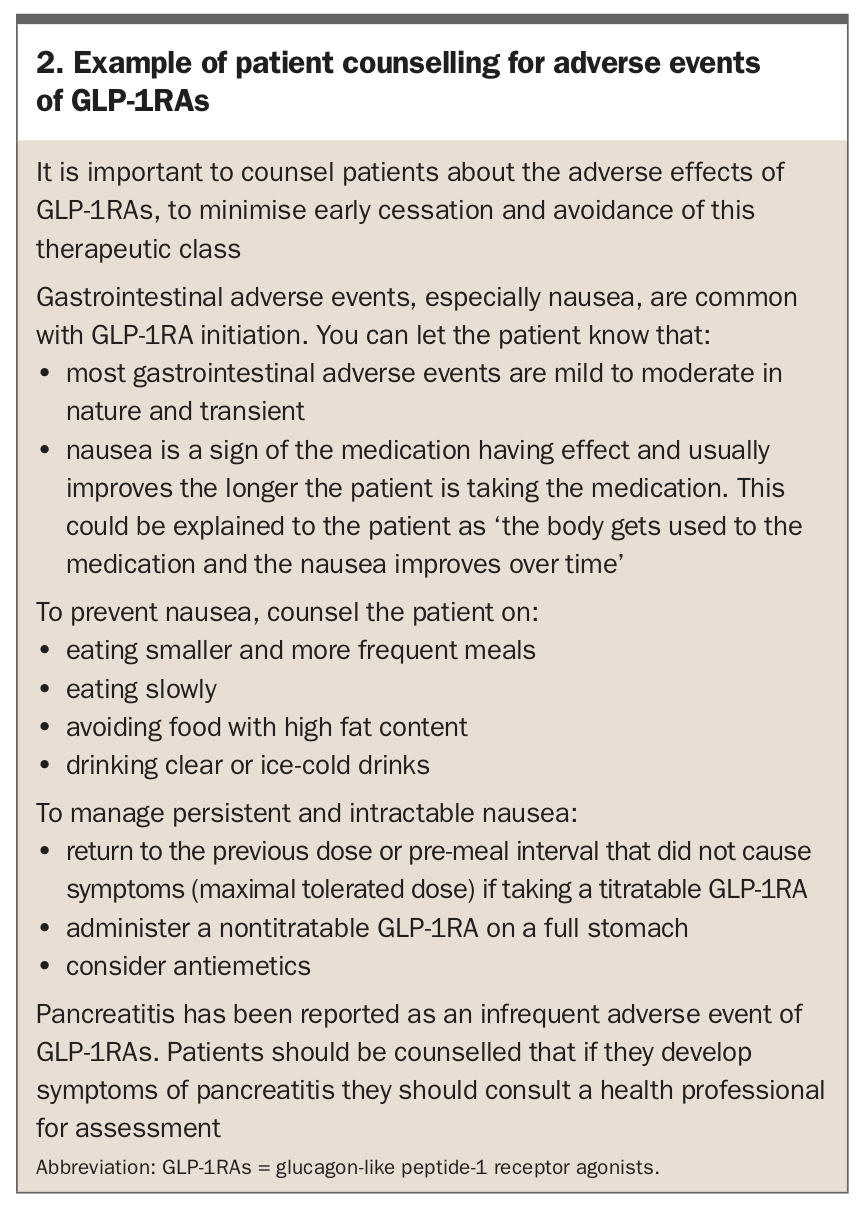
Following the decision to prescribe a GLP-1RA, the patient should be counselled on injection techniques, dose titration, expected adverse effects (see Box 2) and when to seek help.
{kind=link}
Injection technique
Currently, GLP-1RAs are only given by subcutaneous injection in Australia. GLP-1RAs may be the first subcutaneous injected medication for insulin-naïve patients and thus advice on safe injection technique is often required.30 The delivery device for dulaglutide does not require the patient to attach a needle and it may therefore be the preferred agent for those who have poor dexterity or are needle phobic. Referral of the patient to a diabetes nurse educator is recommended for injection technique education.
Dose titration
Depending on the chosen agent, patients may need educating on the dose titration schedule (Table).
- Dulaglutide is only given at the one dose of 1.5 mg once weekly at any time of day, independent of meals.31
- Exenatide should be started at a dose of 5 mcg twice daily for four weeks and can then be uptitrated to 10 mcg twice daily. It can be administered at any time within the 60 minutes before the two main meals of the day, more than six hours apart. If an injection is missed before a meal, exenatide should be administered with the next scheduled dose, rather than after a meal.32
- Semaglutide requires a slow uptitration of the dosage, initially starting at 0.25 mg once weekly for four weeks then uptitrated to 0.5 mg once weekly. After four weeks, the dose can be increased to 1 mg once weekly to optimise glycaemic control. The maintenance dose should be the highest tolerated dose for the patient (e.g. 0.5 mg once weekly if 1 mg once weekly is not tolerated).33
Adverse effects
The most common adverse effects of GLP-1RAs are gastrointestinal, which are usually mild to moderate and transient. In particular, nausea (affecting up to 50% of patients) and diarrhoea (more than 10%) are very common, and vomiting, abdominal pain, dyspepsia and constipation (1 to 10%) are common.34 It is imperative to counsel the patient that nausea is expected, is a sign of the medication having effect and usually improves the longer a patient is taking the medication. This could be explained to the patient as ‘the body gets used to the medication and the nausea improves over time’. Nausea can potentially be prevented by making dietary changes, such as eating smaller and more frequent meals, eating slowly, avoiding food with high fat content, and drinking clear or ice cold drinks.35 Nausea can be addressed in several of different ways:
- if receiving a titratable GLP-1RA, return to the previous dose or premeal interval that did not cause symptoms (maximal tolerated dose)
- give a nontitratable GLP-1RA on a full stomach
- consider antiemetics for intractable symptoms.
Diarrhoea can be managed by reducing consumption of milk and milk products, avoiding food with a high fat content and drinking plenty of fluids.35
Pancreatitis has been reported as an infrequent adverse event of GLP-1RA therapy (although no significant increase was found in cardiovascular outcome trials). Patients should be counselled that if they develop symptoms of pancreatitis they should consult a health professional for assessment.
Although use of GLP-1RAs does not increase the risk of severe hypoglycaemia,10 it may elevate the risk of hypoglycaemia caused by insulin and sulfonylureas if prescribed with these agents.36 If patients are already close to their glycaemic target before starting GLP-1RAs, the dose of their other antihyperglycaemic medications, especially insulin and sulfonylureas, may need to be decreased at GLP-1RA prescription, to prevent hypoglycaemia. For example, a patient taking once-daily long-acting (basal) insulin and starting a weekly GLP-1RA could be instructed ‘after the second injection of dulaglutide/ semaglutide, every time your fasting glucose level is below [target] mmol/L, reduce your [insulin brand] insulin dose by [10% of dose] units’.
In addition, GLP-1RAs reduced systolic blood pressure by a range of 1.84 mmHg (95% CI −3.48 to −0.20) to 4.60 mmHg (95% CI −7.18 to −2.03) in a meta-analysis.37 After a patient starts GLP-1RAs their blood pressure should be monitored and the dose of antihypertensives may need to be reduced.
Phase 3. First follow-up consultation
After a patient starts GLP-1RAs, it is important to follow up to assess tolerability and injection technique. We recommend conducting this review between two and four weeks after the patient starts taking the GLP-1RA. As nausea is a common side effect, dietary changes should be reviewed vigilantly. If nausea is intolerable, the dose of the current agent may be reduced (if possible) or another class of GLP-1RA may be trialled. Injection technique issues and injection site reactions should be assessed. Glycaemic efficacy, including hypoglycaemia and hyperglycaemia, should be evaluated with measurement of blood glucose level and HbA1c at three months, especially if the doses of other antihyperglycaemic agents were reduced or ceased. Blood pressure should be assessed for consideration of a reduction in the dose of antihypertensives. The early impact on body weight can also be assessed at this time.
Phase 4. Unmet target
Despite the glycaemic efficacy and related benefits of GLP-1RAs, some patients may not achieve their target HbA1c after four to six months of use, by which time the full effects of the medication would be manifest. If adherence and injection technique are confirmed, it is important to consider the available algorithms to prescribe additional or alternative therapy.1,6,7 Options include SGLT-2 inhibitors, which also have cardiorenal protective benefits, or sulfonylureas.38 DPP-4 inhibitors should not be prescribed together with GLP-1RAs, as the combined incretin therapy has no significant synergistic effects and is not cost effective.39 Concurrent use of a GLP-1RA and SGLT-2 inhibitor is safe and effective;40 however, this combination is not subsidised by the PBS. Depending on the HbA1c and comorbidities, specialist advice may be needed at this time.
Conclusion
GLP-1RA medications should be considered in all eligible patients with type 2 diabetes whose HbA1c is not at their individualised target, who have established atherosclerotic cardiovascular disease or who have a compelling need to promote weight loss or minimise hypoglycaemia. However, major precautions and contraindications should be considered and patients appropriately counselled on injection techniques, expected adverse effects and dose titration regimens. The practical advice outlined in this article should help GPs to prescribe GLP-1RAs safely and effectively and ensure patients benefit from these new potent and multifaceted agents. ET