Gestational diabetes: current and future directions

Dr Pavey is an Endocrinologist at Mater Health Brisbane. Professor David McIntyre is Head of Mater Clinical Unit at The University of Queensland, Brisbane; and Director of Obstetric Medicine, Mater Health Brisbane, Qld.
Diabetes and pregnancy
Health problems in pregnancy
Debate and uncertainties on the diagnosis of gestational diabetes mellitus (GDM) still exist, with no single process or set of diagnostic criteria accepted globally. Despite this, the prevalence of GDM continues to rise. More recent evidence shows that GDM is a risk factor for poor metabolic health in both the mother and offspring. Clinicians should therefore approach pregnancy and the postpartum period as an opportunity to implement preventive healthcare measures to avoid or delay impending metabolic and cardiovascular disease.
- The diagnostic process and criteria for gestational diabetes mellitus (GDM) are not universal, with debate ongoing about which method is best.
- The threshold for diagnosing GDM in early pregnancy remains unclear.
- Despite variable diagnostic processes and criteria, the prevalence of GDM is increasing over time, in line with the overweight and obesity epidemic and advancing maternal age. This has been compounded by changes to the diagnostic criteria.
- Metformin use in pregnancy is common although remains controversial because it crosses the placenta, therefore, there is potential for concern to the developing fetus.
- Pregnancy is a stress test for a woman’s future risk of cardiovascular and metabolic disease. GDM is a risk factor for developing future type 2 diabetes and cardiovascular disease, as early as the first decade postpartum.
- Appropriate education and screening postpartum are needed to minimise the future risk of cardiovascular and metabolic disease.
- Treatment of GDM improves perinatal outcomes. Although offspring of women with GDM are at higher risk of adiposity and impaired glucose metabolism, there is no evidence that current treatment of GDM reduces offspring risks.
Gestational diabetes mellitus (GDM) is one of the most common medical complications of pregnancy and its prevalence is increasing globally. Hyperglycaemia in pregnancy is associated with excessive fetal growth and increased rates of primary caesarean birth, neonatal hypoglycaemia and hypertensive disorders of pregnancy. Despite being recognised and treated for many decades, controversy and debate remain on how best to define the diagnosis of GDM. In the past two decades, the landmark Hyperglycaemia and Adverse Pregnancy Outcome (HAPO) study and its follow-up study have provided evidence on the short- and long-term risks of GDM and redefined the diagnostic process.1,2 Additionally, there is increasing evidence that GDM is a risk factor for future maternal and offspring cardiometabolic disease.
Diagnosis of GDM: the ongoing debate
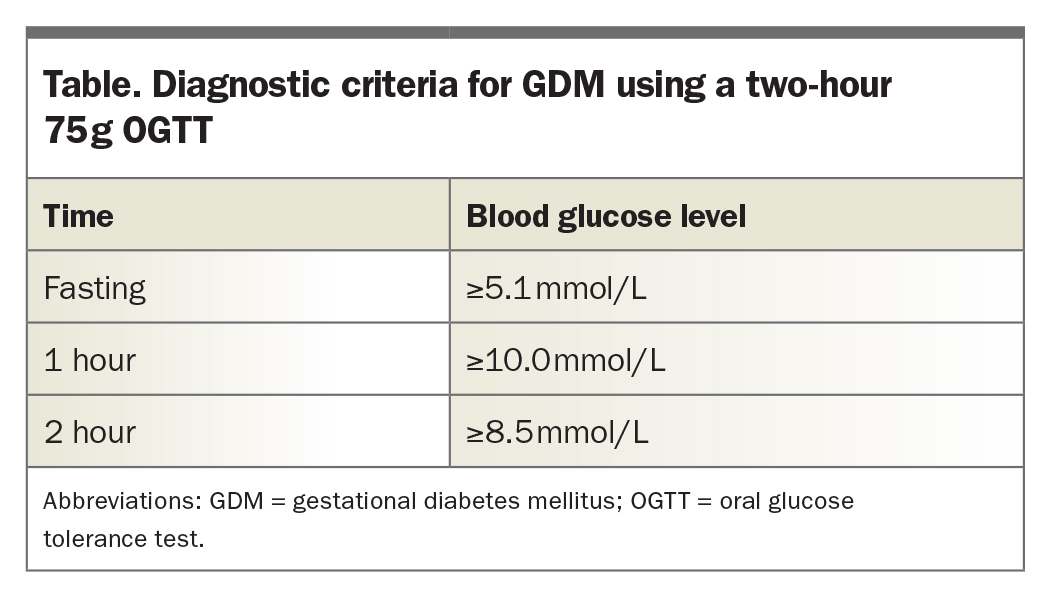
Over the past decade, there has been a refinement in the diagnostic criteria for GDM, without universal acceptance of any one approach internationally. This shift followed the landmark HAPO study findings, which showed a linear increase in adverse pregnancy outcomes (including large-for-gestational-age, neonatal hypoglycaemia, primary caesarean section and preterm delivery) with increasing hyperglycaemia.1 Because of the linear nature of this relationship, it was challenging to establish dichotomous thresholds for fasting, one- and two-hour blood glucose values after an oral glucose load. Instead, a consensus panel opted for an adjusted odds ratio of 1.75 times the mean for the diagnostic thresholds, considering large-for-gestational-age, increased fetal adiposity and neonatal hyperinsulinaemia as outcomes. This has led to the current diagnostic criteria for GDM using a 75 g oral glucose tolerance test (OGTT), as summarised in the Table. This ‘one-step’ process and criteria were endorsed by the Australasian Diabetes in Pregnancy Society (ADIPS) in 2014; however, there is still much debate globally about their acceptance. The arguments against the one-step process include an increased frequency of GDM and the additional burden that this places on healthcare resources. This, however, needs to be weighed up against the overall short- and long-term health and economic benefits associated with treating GDM, from reduced perinatal complications to the opportunity for preventing and delaying the onset of type 2 diabetes, obesity and cardiovascular disease.
{kind=link}
A 2021 US pragmatic randomised controlled trial that compared the one-step versus two-step model (consisting of a nonfasting 50 g glucose challenge, followed by 100 g OGTT if positive) for diagnosis has reinvigorated the debate.3 This trial reported no benefit of the one-step diagnostic process (as endorsed by ADIPS and the International Association of Diabetes and Pregnancy Study Groups [IADPSG]) compared with the two-step process (which is commonly used in the US) in terms of perinatal outcomes.3 The trial has attracted criticism for several reasons. The trial design allowed providers the option of choosing which diagnostic strategy to use, rather than complying with the randomly allocated strategy.4 Only two-thirds of women in the one-step group received their allocated testing strategy compared with 92% in the two-step approach.4,5 In addition, the rates of pharmacotherapy use were similar in both groups, suggesting the additional GDM cases detected with the one-step IADPSG approach did not have trivial hyperglycaemia.4 A necessary question for future research is whether the considerable group of women who are ‘one-step positive/two-step negative’ and their offspring achieve a reduction in the short- and long-term adverse outcomes from treatment of GDM.
The COVID-19 pandemic has led to temporary changes to screening for GDM because of concerns of potentially exposing a pregnant woman to COVID-19 for two to three hours at a collection facility at a peak time of day. In Australia, a revised two-step process with an initial fasting blood glucose test, followed by a full 75 g OGTT if the fasting glucose level was between 4.7 and 5.0 mmol/L was recommended during the pandemic. Fasting glucose levels of 4.6 mmol/L or below excluded GDM and 5.1 mmol/L or above was considered diagnostic. This method misses the diagnosis of GDM in 4 to 46% of cases; however, this subpopulation of mothers with GDM may not have any increase in adverse outcomes compared with women without GDM.6,7 Although currently this diagnostic process is not recommended outside of the COVID-19 pandemic context, it does pave the way for future research into changing the diagnostic pathway.
Additionally, measurement of alternative biomarkers of glucose metabolism may help predict pregnancy-induced glucose intolerance without the need for an OGTT. Measurement of glycated haemoglobin (HbA1c) levels has not proven useful in routine GDM diagnosis. Plasma-glycated CD59 appears promising as a novel biomarker for GDM, but further prospective research is required.8
Classifying early GDM
Uncertainty remains around the definition of normal and abnormal glucose levels in early pregnancy. ADIPS and IADPSG have recommended using the standard GDM thresholds and testing approach, although there are no data supporting this and IADPSG subsequently withdrew this recommendation. Fasting glucose levels decrease in early pregnancy and studies have shown that using a fasting plasma glucose level of 5.1 mmol/L or more in early pregnancy leads to high false-positive detection rates. An early pregnancy threshold should perhaps be 6.1 mmol/L or more, but this requires further validation.9
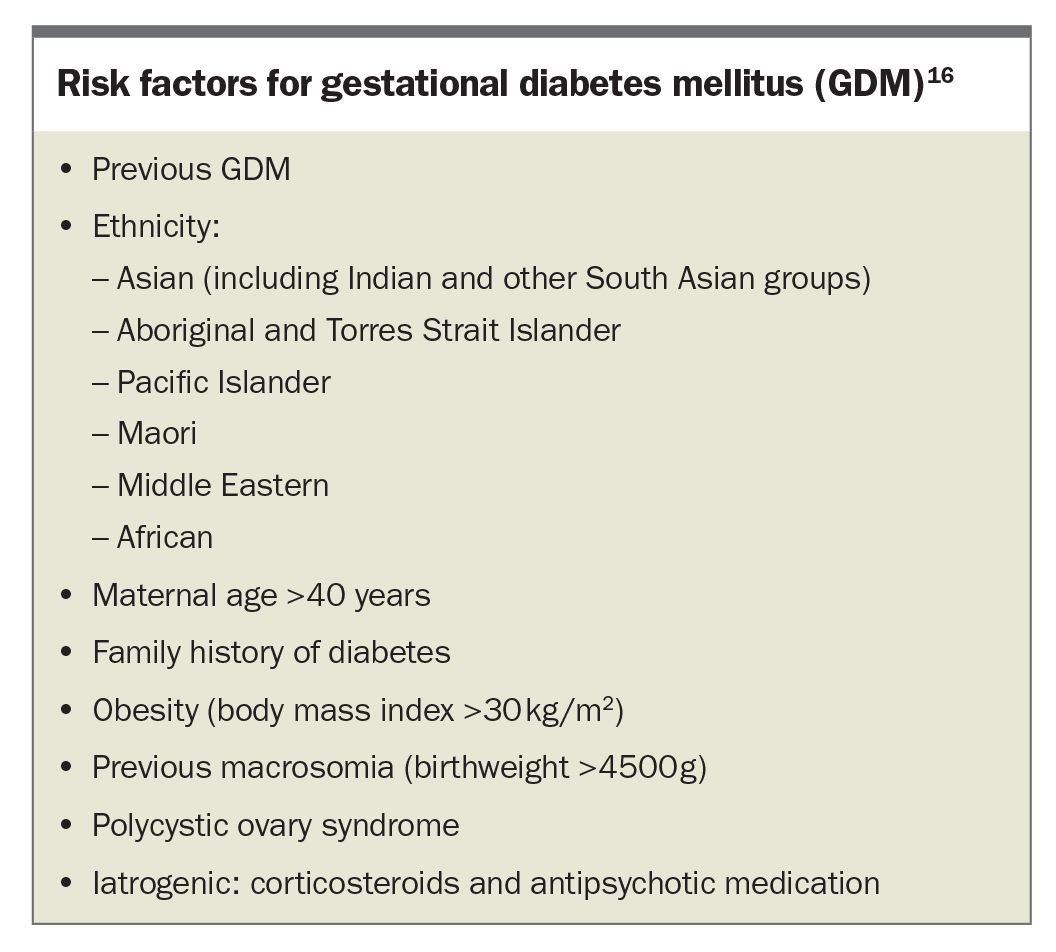
The Australian multicentre, randomised controlled Treatment of Booking Gestational Diabetes Mellitus (TOBOGM) study is underway, which seeks to determine if there is benefit in treating early GDM and which diagnostic thresholds should be considered. These results may also have implications for the current diagnostic GDM criteria at 24 to 28 weeks, as the studies underpinning this trial include women who fulfil early GDM criteria. Until further data are available, current Queensland and Australian guidelines recommend that high-risk women (see Box) should be screened in the first trimester with an OGTT (using the same diagnostic thresholds as for 24 to 28 weeks, see the Table) or an HbA1c level of more than 5.9%.10,11
{kind=link}
The changing prevalence of GDM
It is difficult to compare the prevalence of GDM globally because of a lack of uniformity in the screening and diagnostic criteria. The prevalence of GDM is reported as 14% in pregnant women in Australia, although this varies widely between regions.12 Prevalence is increasing in Australia and worldwide, with studies showing a 1.03 to 3.78-fold rise in prevalence after the adoption of the IADPSG criteria.13 Data from the National Diabetes Service Scheme shows GDM is continuing to rise, with a 12% increase in women registered with GDM in the past 12 months ending in March 2022.14 The rise in prevalence cannot be attributed to a change in criteria alone, however, as a rising national trend was evident in Australia before the implementation of these guidelines in 2015.
Contributing factors to the increasing prevalence of GDM include:
- advancing maternal age, with the average maternal age increasing by almost four years in the past four decades to 30.8 years15
- increasing rates of maternal overweight and obesity. In line with the increases in national overweight and obesity rates, almost half of pregnant women in Australia are now considered to be overweight or obese.16 This is in addition to a population-wide increase in diabetes prevalence12
- changes in ethnic diversity, with increases in the populations/ethnic groups known to have a high risk of GDM and type 2 diabetes, namely those born in southern and central Asia, Southeast Asia, North Africa and the Middle East.16
With increasing prevalence of GDM, innovative solutions to education and management including novel technological solutions are needed to ensure ongoing adequacy of care can be maintained.
Long-term effects of in utero metformin exposure
Metformin use in pregnancy is controversial, as shown by its variable use among healthcare services in different countries.17 Unlike insulin, metformin crosses the placenta, therefore, there is potential for concern to the developing fetus. Use of metformin has been shown to have glycaemic and immediate neonatal outcomes comparable to insulin in randomised controlled trials, with lower birth weights than those treated with insulin without an increased risk of small-for-gestational-age (birth weight less than tenth percentile).18,19 However, use of metformin appears to be associated with accelerated postnatal growth at 18 to 24 months of age, with a mean weight difference of 440 g compared with offspring of mothers treated with insulin and, in particular, increased subcutaneous fat localised to the arm.19,20 Longer-term follow up has demonstrated a higher body mass index (BMI) by age 5 to 9 years (BMI mean difference 0.78 kg/m2); however, absolute weight and height difference did not reach statistical significance.19 Higher abdominal and visceral fat volumes were seen in children exposed to metformin (measured by an MRI), however, no significant differences were seen in total fat mass or abdominal mass (measured by dual-energy x-ray absorptiometry) suggesting this finding is ambiguous. Longitudinal studies are ongoing and will hopefully guide recommendations for the use of metformin in pregnancy.
Prevention of future cardiometabolic disease
Pregnancy, with its resultant physiological adaptations, is a biological stress test for the mother and allows the identification of increased risks for future adverse maternal health conditions. Clinicians should therefore approach pregnancy and the postpartum period as an opportunity to implement preventive healthcare measures to avoid or delay impending metabolic and cardiovascular disease. It is well established that GDM is a risk factor for developing future type 2 diabetes, with a sevenfold increased risk of developing type 2 diabetes in the first decade after pregnancies complicated by GDM compared with women with normoglycaemic pregnancies.21 Multiparity, insulin requirement in pregnancy, preterm delivery, advanced maternal age and higher values on screening OGTT and HbA1c are associated with this heightened risk.22 GDM is also associated with an increased risk of other major medical conditions, including cardiovascular disease, chronic kidney disease, advanced liver disease, female malignancies (ovarian, uterine, cervical and breast cancer), glaucoma and retinopathy.21 Chronic kidney disease, advanced liver disease and ophthalmological outcomes are dependent on the development of type 2 diabetes, however, cardiovascular disease is not. GDM is associated with a twofold increased risk of developing cardiovascular events in the first decade postpartum.23
Although pregnancy and the postpartum period offer an opportunity to provide education and preventive measures to reduce the long-term risks associated with GDM, adherence to postpartum screening is poor. There are several hurdles to the implementation of postpregnancy follow up. Glucose intolerance typically resolves immediately postpartum, therefore, women may believe there are no lasting effects. The treating clinician needs to find a balance between providing reassurance that GDM will resolve postpartum and emphasising concerns about ongoing associated health risks. Moreover, the significant adjustment of caring for a new baby often supersedes the mother’s focus on her own wellbeing.
Healthcare providers report multiple barriers, including patients being lost to follow up or being unaware of the implications of a GDM diagnosis for long-term health, as well as inconsistent guidelines on appropriate follow up.24 A lack of communication between maternity healthcare providers and GPs is also contributory.24 Finding local healthcare system-specific and culturally appropriate ways to overcome these barriers is needed to help reduce the risk of metabolic and cardiovascular disease in these women. Mothers are likely to attend healthcare services that are focused on their baby’s wellbeing, including vaccination programs and growth and developmental assessments, which often occur at regular intervals for at least five years. Linking maternal postpartum follow up with routine child health reviews may improve preventive health opportunities.
Breastfeeding has been shown to reduce the risk of progression of GDM to type 2 diabetes, with greater benefit derived from more intense and a longer duration of lactation.25 Breastfeeding has also been associated with lower rates of hypertension, dyslipidaemia and cardiovascular disease and should be encouraged whenever possible.26 Unfortunately, women with GDM are less likely to breastfeed and do so for a shorter duration than their peers, with even lower rates reported in those who required insulin therapy during pregnancy or who are obese.27 Fortunately, consistent support, if available, increases rates of breastfeeding. In addition to breastfeeding, both lifestyle interventions and use of metformin can reduce progression to overt diabetes by about 50%.28 These factors provide great potential to prevent or delay type 2 diabetes and cardiovascular disease in women with a history of GDM.
GDM confers to the infant an increased risk of adiposity and impaired glucose metabolism as shown in follow-up studies that span out to 11 years of age.2 Unlike future maternal risks, at present there is unfortunately no evidence that treatment of GDM, according to current protocols, prevents these offspring complications and interrupts the vicious cycle of intergenerational metabolic disease transmission.21 Longer-term results are awaited.
Preparing for future pregnancies
GDM is a risk factor for recurrence in future pregnancies, with a meta-analysis in 2015 showing a pooled GDM recurrence of 48%.29 Focusing on ways to minimise the risk of recurrence potentially has the ability to reduce the established complications of hyperglycaemia in pregnancy. Dietary intervention and physical activity before and in early pregnancy is associated with a lower risk of GDM.30 During pregnancy, the timing of lifestyle interventions (diet, physical activity or both) appears to be key, with evidence that intervention before the 15th gestational week can help reduce the risk of GDM.31 The overall quality of evidence for lifestyle intervention has been assessed as moderate in a 2020 Cochrane review.32 Low-quality evidence suggests that myo-inositol and vitamin D supplementation during pregnancy may be of benefit in reducing the risk of developing GDM, however, randomised controlled trials are needed to confirm these findings.32 A large, population-based study reported that a 10% difference in prepregnancy BMI is associated with a lower risk of pregnancy complications including GDM, pre-eclampsia, macrosomia and stillbirth.33 Therefore, focusing on an achievable weight loss goal in the interpregnancy period may lead to improved perinatal outcomes.
Conclusion
Diagnosis of GDM remains a contentious topic with no single process or set of diagnostic criteria accepted globally. Prevalence of GDM has increased with the introduction of the IADPSG one-step approach. Key additional underlying contributors are the increasing rates of prediabetes and obesity in women of childbearing age. More recent evidence shows that GDM is a risk factor for poor metabolic health in both the mother and offspring. This represents an opportunity for improving maternal health, but unfortunately co-ordinated preventive measures are rarely instituted. Further, despite evidence of risk to the offspring, current evidence suggests that current treatment of GDM does not affect their long-term outcomes. Addressing postnatal preventive health is of paramount importance to minimise future maternal and offspring cardiometabolic disease. ET
COMPETING INTERESTS: Dr Pavey: None. Professor McIntyre has received payment or honoraria from Mead Johnson and Philips Healthcare and support for attending meetings and/or travel from Danish Diabetes Academy. He is also on the International Federation for Gynaecology and Obstetrics – pregnancy and long term health committee.