Optimising bone health during endocrine therapy for hormone sensitive cancer


Bone diseases
Cancer chemotherapy
As survival rates of patients with breast and prostate cancer increase, the need to address long-term adverse effects of cancer treatment on skeletal health is a priority to long-term survivorship. An individualised approach to assessment and management of all patients receiving endocrine therapy includes a baseline fracture risk assessment and ongoing surveillance. Targeted lifestyle changes and pharmacological therapies can help optimise skeletal health.
- Endocrine therapies for breast and prostate cancer are effective at reducing cancer recurrence but may have adverse skeletal effects that need to be appropriately assessed and managed to optimise benefit.
- Screening, surveillance and management of skeletal health should be tailored to the individual and involve a multidisciplinary team consisting of oncologists, endocrinologists, GPs, physiotherapists and exercise physiologists.
- Adequate dietary calcium, vitamin D and targeted exercise are recommended for all patients receiving endocrine therapy.
- For suitable patients, antiresorptive therapies have been shown to reduce bone mineral density loss, with some evidence of fracture risk reduction.
Breast and prostate cancer are among the most common malignancies in women and men, respectively. Endocrine therapy, an essential part of the armamentarium for the treatment of hormone sensitive breast and prostate cancer, exerts adverse effects on the skeleton and is associated with accelerated bone loss, microstructural decay and increased fracture risk. Fragility fractures are associated with devastating consequences to the individual, such as increased mortality and morbidity, and are also associated with a high socioeconomic burden. As such, preservation of bone health is a key long-term survivorship priority. In this review, we describe how endocrine therapies for breast and prostate cancer affect bone health and outline management strategies to mitigate endocrine therapy-induced bone loss and prevent fragility fractures.
Endocrine therapy for breast cancer
Around 80% of breast cancers are oestrogen-receptor positive and respond to endocrine therapies. Current endocrine therapies inhibit oestradiol-mediated effects on breast cancer progression in one of two ways – they deplete circulating oestradiol by blocking aromatase (aromatase inhibitors, AIs) or they competitively inhibit binding of oestradiol to the oestrogen receptor (ER) in breast tissue (selective oestrogen receptor modulators, SERMs, most commonly tamoxifen). The choice of therapy depends on the woman’s menopausal status, cancer characteristics and contraindications to a particular type of treatment.
AIs have shown superior efficacy to tamoxifen in preventing tumour recurrence and reducing mortality in postmenopausal women, and are generally used as first-line therapy for five years.1 Treatment with AIs is now being extended to 10 years in suitable women with high-risk features, based on clinical trial evidence of a modest reduction in breast cancer recurrence with extended therapy.2 In premenopausal women, tamoxifen is first-line. However, in those who are at higher risk of tumour recurrence, the use of gonadotropin releasing hormone (GnRH) analogues (which suppress ovarian oestradiol production) in combination with tamoxifen improves disease-free survival compared with tamoxifen alone, with further improvements observed with the combination of GnRH analogues and the AI exemestane.3,4 Of importance, AIs cannot be used as monotherapy in premenopausal women because oestradiol depletion reduces negative feedback on the gonadal axis, stimulating further oestradiol production. The use of AIs in this context requires concurrent ovarian function suppression, either with concurrent use of GnRH analogues, bilateral oophorectomy or radiotherapy to both ovaries.
In postmenopausal women, AIs increase bone remodelling, producing about a twofold increase in bone loss compared with age-matched postmenopausal women who are not being treated with AIs. Bone loss is most marked in the first one to two years after starting endocrine therapy and is particularly evident at the lumbar spine. In a large meta-analysis, women treated with AIs had a 17% (95% confidence interval [CI], 1.07 to 1.28) higher fracture risk than women not being treated with AIs and a 35% (95% CI, 1.21 to 1.51) higher fracture risk compared with women treated with tamoxifen.5 However, fracture was not a primary endpoint in these trials and fracture risk was likely to have been underestimated due to under-reporting. Owing to significant confounding in currently available data, there is insufficient evidence to determine whether fracture rates return to baseline once the AI is stopped.
Premenopausal women treated with ovarian function suppression with or without concurrent tamoxifen or an AI experience the largest magnitude of lumbar spine bone mineral density (BMD) loss at 12 months (8.2% with GnRH monotherapy, 9.3% with GnRH/AI and 5.6% with GnRH/tamoxifen).6,7 The implications of this bone loss for future fracture risk are undetermined.
Tamoxifen as monotherapy has different effects on the skeleton depending on ovarian oestradiol production. In postmenopausal women, tamoxifen acts as a partial ER agonist in bone and produces an increase in BMD, in contrast to its antagonistic effects in breast tissue, with conflicting results observed for fracture risk.5,8,9 In premenopausal women, in whom circulating levels of oestradiol are higher, tamoxifen acts as a ER partial antagonist in bone and causes bone loss, although this effect is modest compared with placebo (annual 1.4% loss versus 0.2% gain in spine BMD).10 When combined with ovarian suppression, tamoxifen reduces the bone loss produced by ovarian suppression.11
Assessment and management
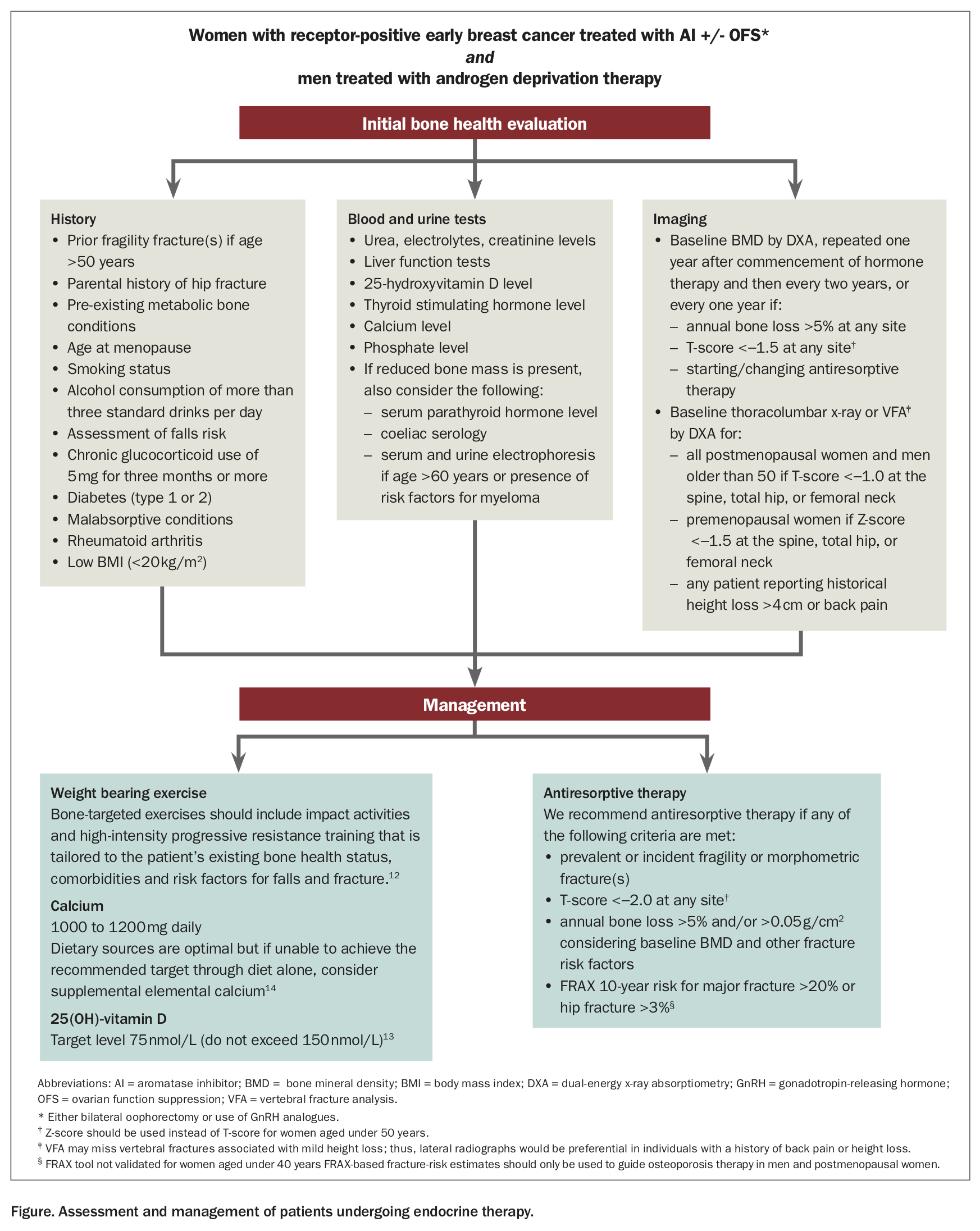
Australian and New Zealand expert consensus guidelines recommend that all women who commence endocrine therapy should have a baseline assessment of their fracture risk, which includes ascertainment of clinical risk factors, basic laboratory testing and BMD measured by dual-energy x-ray absorptiometry (DXA) (Figure12-14).15 Of note, there is currently no MBS item number for DXA scanning for female hypogonadism for those aged over 45 years. Women aged under 45 years or 70 years and over are eligible for an initial DXA scan under item numbers 12312 and 12320, respectively, with subsequent scans using other clinically appropriate MBS item numbers. Women with osteopenia should have vertebral imaging with vertebral fracture analysis at the time of DXA scanning, or with a formal lateral thoracolumbar spine x-ray to exclude occult osteoporotic vertebral fracture (Figure). The utility of bone turnover makers has not been established and they should not be measured routinely. Fracture risk assessment tools, such as the Fracture Risk Assessment Tool (FRAX) (www.sheffield.ac.uk/FRAX/) or the Garvan Institute’s fracture risk calculator (www.garvan.org.au/promotions/bone-fracture-risk/calculator/), may not offer accurate fracture risk prediction as they have not been validated in women aged under 40 years and in those with breast cancer who are receiving AIs. Skeletal health should be monitored at least throughout the duration of endocrine therapy. There is insufficient data to make firm recommendations regarding frequency of monitoring, although the expert recommendation is to repeat testing after 12 months of endocrine therapy and then individualise monitoring based on the woman’s overall fracture risk.15
{kind=link}
All women should be advised to adopt lifestyle changes that promote skeletal and overall health. Based on evidence outside the breast cancer population, adequate calcium intake preferably through dietary sources, correction of 25-hydroxyvitamin D (25[OH]D) deficiency, smoking cessation and bone-targeted exercise should be recommended (Figure). Bone-targeted exercises include impact activities and high-intensity progressive resistance training, which should be tailored to the patient’s existing bone health status, comorbidities and risk factors for falls and fracture.12 Bisphosphonates or denosumab are considered first-line treatment for women who are at sufficient risk of fracture to warrant pharmacotherapy (Figure). In postmenopausal women, all currently available antiresorptives prevent AI-induced BMD loss, and antifracture efficacy has been established for denosumab. Compared with placebo, denosumab 60 mg administered six-monthly for 36 months reduced clinical fractures by 50% (95% CI, 0.39 to 0.65, absolute fracture incidence 9.6% denosumab arm vs 5.0% placebo arm).16 If denosumab is stopped, follow-on bisphosphonate therapy is necessary, as denosumab cessation without follow-on bisphosphonate therapy is associated with rapid bone loss and increased fracture risk.17 In premenopausal women, zoledronic acid 4 mg administered six-monthly prevents GnRH/AI combination-induced BMD loss; however, data on denosumab are not available.6
Of note, there is no PBS item number for antiresorptive therapy specific to the use of endocrine therapy. Guidelines recommend consideration of antiresorptive therapy if annual bone loss during endocrine therapy exceeds 5% and/or 0.05 g/cm2 or for T-scores below −2.0. Prescription of antiresorptive treatment outside of the current PBS subsidised indication (for women with a prior fragility fracture or women 70 years or older who have a DXA BMD T-score <−2.5) requires a detailed discussion between the treating specialist and the women who fulfill guideline criteria but do not meet criteria for PBS subsidy.
Use of antiresorptives as adjuvant therapy to improve oncological outcomes is beyond the scope of this article. Current TGA approved anabolic therapies for postmenopausal osteoporosis, teriparatide and romosozumab, are not approved for use in women with breast cancer due to insufficient efficacy and safety data. There is a theoretical concern that parathyroid hormone analogues such as teriparatide may stimulate cancer progression. Teriparatide is also contraindicated in patients who have received radiation therapy that may have involved any part of the skeleton, due to an association with osteosarcoma in rodent studies, although the rate of osteosarcoma in human studies is consistent with background rates.
Androgen deprivation therapy for prostate cancer
Nearly 50% of men diagnosed with prostate cancer receive androgen deprivation therapy (ADT).18 ADT is used as an adjuvant treatment for men undergoing curative-intent radiotherapy, under specific circumstances for men with biochemical relapse (i.e. prostate-specific antigen increase) after treatment with curative intent and for men with symptomatic metastatic prostate cancer.19,20 ADT is most commonly achieved through the use of GnRH analogues, which suppress the hypothalamic-pituitary-testicular axis so that serum testosterone and, therefore, circulating oestradiol concentrations fall to near zero.
The profound sex steroid deficiency induced by ADT causes accelerated bone loss and increased fracture risk. A meta-analysis of prospective cohort studies of men with prostate cancer receiving ADT reported lumbar spine and total hip BMD decline over 12 to 36 months compared with nonprostate cancer control groups.21 The rate of bone loss appears to be greatest in the first 12 months of ADT and has been reported to occur at a rate five- to 10-fold that of healthy controls.22 Records from over 50,000 men in a US registry clinical database found that one fracture was seen over the period of one to five years after diagnosis for every 28 men exposed to a GnRH analogue in the first year of treatment.23 In registry data from over 80,000 men, the adjusted hazard ratio for death after an ADT-associated fracture was 2.05 (95% CI, 1.98 to 2.12).24 It is important to note that, especially after prolonged 18 to 36 months of ADT, recovery of the gonadal axis after cessation of ADT can take a long time and is not guaranteed. Any such persisting hypogonadism represents an ongoing risk factor for fracture.
Assessment and management
Men receiving ADT should have a baseline measurement of BMD and fracture risk (Figure). This includes assessing traditional risk factors for osteoporotic fracture including smoking, excessive alcohol consumption, long-term glucocorticoid exposure, falls, 25(OH)D deficiency and inadequate dietary calcium intake. Absolute fracture risk calculators such as FRAX or Garvan Institute’s fracture risk calculator are recommended, with the caveat that they may underestimate fracture risk in men receiving ADT.25 In using the FRAX tool, ADT should be considered a cause of secondary osteoporosis.26 Men with osteopenia should have vertebral imaging with vertebral fracture analysis at the time of DXA scanning, or with a formal lateral thoracolumbar spine x-ray to exclude occult osteoporotic vertebral fracture (Figure).27 An annual DXA scan and fracture assessments are recommended for the first two years of ADT and then individualised with ongoing monitoring continued while men remain hypogonadal.27 There is no proven clinical benefit for the monitoring of bone turnover markers.
Men with inadequate vitamin D status should receive supplementation (loading then maintenance dosing) to achieve a 25(OH)D concentration of 75 nmol/L.13,26,28 Calcium supplementation to achieve a total calcium dose of 1000 to 1200 mg per day is recommended only if dietary calcium intake cannot achieve this level. 26,29 Exercise has established benefits on body composition, muscle function and quality of life in men undergoing ADT, but it has not been definitively shown to prevent loss of BMD and there are no data to show effectiveness in fracture prevention.30,31
Extrapolating from recommendations for the noncancer population, antiresorptive medication is indicated for men with:
- osteoporosis, defined by a T-score below −2.5 at the total hip, femoral neck or lumbar spine, and/or prior fragility fracture
- a calculated 10-year absolute osteoporotic fracture risk of 20% or higher for major osteoporotic fracture or 3% or higher for hip fracture (based on (US) cost-effectiveness data).26,32,33
Not all such men will be eligible for a PBS subsidy. Australian guidelines additionally recommend antiresorptive therapy for primary prevention of fracture in men with a T-score of −2.0 or lower.27 Guidelines support the use of oral or intravenous bisphosphonates or denosumab in standard osteoporosis doses.26,27,29
All available bisphosphonates are effective in preventing BMD decline in men receiving ADT, but zoledronic acid is most strongly supported by evidence. No individual published trials demonstrate fracture prevention efficacy for bisphosphonates in traditional osteoporosis doses. A meta-analysis of 15 trials of bisphosphonates, ranging in duration from six to 36 months, showed the number needed to treat (NNT) to prevent one fracture was 166.6 for bisphosphonates overall and 14.9 for zoledronic acid.34 The analysis was heavily influenced by two studies using three-weekly zoledronic acid to prevent skeletal-related events in men with castrate-resistant metastatic prostate cancers, and the proportion of nonpathologic fractures in these trials is not clear. Pooled risk ratios for fracture from trials in nonmetastatic prostate cancer did not show definitive fracture reduction.
More definitive data are available for denosumab. A placebo-controlled trial of 1468 men receiving ADT (mean age 75 years, baseline femoral neck T-score −1.5, 25% with a prior osteoporotic fracture) showed six-monthly denosumab 60 mg improved BMD at the lumbar spine and femoral neck at 24 months and prevented new radiological vertebral fracture over 36 months, with an NNT of 42.35 Higher dose denosumab, 120 mg four-weekly, is used to prevent skeletal-related events in men with bone metastases due to castrate-resistant prostate cancer. Importantly, once started, denosumab cannot be stopped without ongoing use of an alternative antiresorptive, because of a rebound increase in bone remodelling and vertebral fracture risk.17
There are no data on the use of the TGA-approved anabolic agents teriparatide and romosozumab for treatment of bone loss or prevention fracture in men with prostate cancer. Neither can be recommended in this context at this time. Teriparatide is contraindicated in the context of active malignancy, and romosozumab may further increase the risk of cardiovascular events in a population already known to be at very high risk.
Conclusion
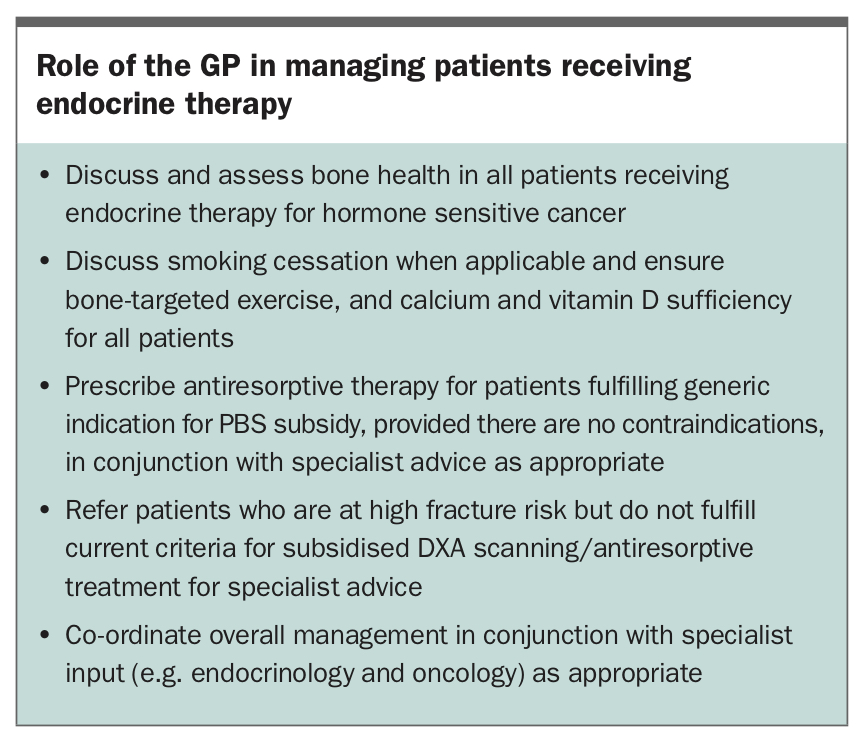
The increasing survival of patients with breast and prostate cancer emphasises the need to address long-term adverse effects of cancer treatment on skeletal health. Patients treated with endocrine therapy experience accelerated bone loss and increased fracture risk. There is a paucity of data to make firm recommendations regarding appropriate fracture risk assessment and ongoing surveillance of bone health in these patients. Nevertheless, all patients receiving endocrine therapy should have a baseline fracture risk assessment and ongoing surveillance, with intervals determined by the individual’s fracture risk and any major changes to their clinical status or therapy. Alongside clinical specialists, GPs have an important role in recognising and helping to manage patients who may be at risk of impaired skeletal health resulting from endocrine therapy (Box).
{kind=link}
Treatment with antiresorptive therapy prevents endocrine therapy-induced bone loss, but may not be PBS reimbursed. Most of these studies are short-term (maximum three years) and do not assess fracture outcomes. The few studies that have assessed fracture outcomes have shown antifracture benefit with denosumab. The efficacy and safety of newer anabolic therapies that have been TGA approved for the treatment of osteoporosis, i.e. teriparatide and romosozumab, have not been established in patients with breast or prostate cancer. Overall, therapeutic hypogonadism in hormone sensitive cancer remains a clinical challenge whereby the benefits and harms of both endocrine and bone-modifying therapy need to be balanced in an individualised approach. ET
COMPETING INTERESTS: Dr Ramchand: None. Dr Russell has received speaker’s honoraria from Amgen. Professor Grossmann has received research funding from Bayer and Otsuka; and speaker’s honoraria from Bayer, Besins Health Care and Novartis.