Assessing for diabetes-related complications

Diabetes complications
Diabetes medicines
The duration of type 2 diabetes is increasing owing to the global trend towards obesity and younger age of onset. In all patients with diabetes, regardless of type, the risk of developing complications is strongly related to disease duration and glycaemic control. People with diabetes need close screening and regular follow up to reduce their complication burden.
- Diabetes poses a significant health burden and has considerable impact on the healthcare system.
- Screening for microvascular and macrovascular complications is recommended for people with either type 1 or type 2 diabetes.
- People with type 1 diabetes should be screened for associated autoimmune conditions.
- Treatment targets, especially glycated haemoglobin level (HbA1c), should be individualised, taking into account relative risk and potential adverse effects.
The global prevalence of diabetes has increased dramatically; in Australia an estimated 1.2 million adults were reported to have diabetes in 2017-18, representing 4.9% of the total population.1 This number continues to rise and poses a significant burden on our healthcare system. Type 2 diabetes is most prevalent, comprising about 85% of cases.
There is a global trend towards younger age of onset of type 2 diabetes, linked to growing rates of obesity. As a result, the duration of this disease in many patients is increasing. Given the known association between disease duration and complications, there is increased risk of developing diabetes-related complications. People with diabetes diagnosed during early or mid-adulthood, in particular, need close screening and regular follow up to reduce their complication burden. In addition, there is the potential for added mental health burden for both young and older people living with chronic disease. Young women with diabetes need the opportunity to discuss reproduction and contraception.
Almost 50% of individuals with newly diagnosed type 2 diabetes have microvascular or macrovascular complications at diagnosis.2 Due to the more acute presentation of type 1 diabetes, complications at diagnosis are less likely. In all patients, regardless of type of diabetes, the risk of developing complications is strongly related to duration of diabetes and glycaemic control.3,4
There is extensive evidence showing that intensive glycaemic management delays onset and slows the progression of microvascular disease in patients with type 1 or type 2 diabetes.3 The United Kingdom Prospective Diabetes Study (UKPDS), Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, Veterans Affairs Diabetes Trial (VADT) and Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial all showed a reduction in myocardial infarction among patients with intensive glycaemic management.4 Intensive diabetes therapy has substantial long-term benefits for the risk of macrovascular and microvascular disease in patients with type 1 diabetes.5 The risk of hypoglycaemia should always be considered when targeting intensive glycaemic control.4
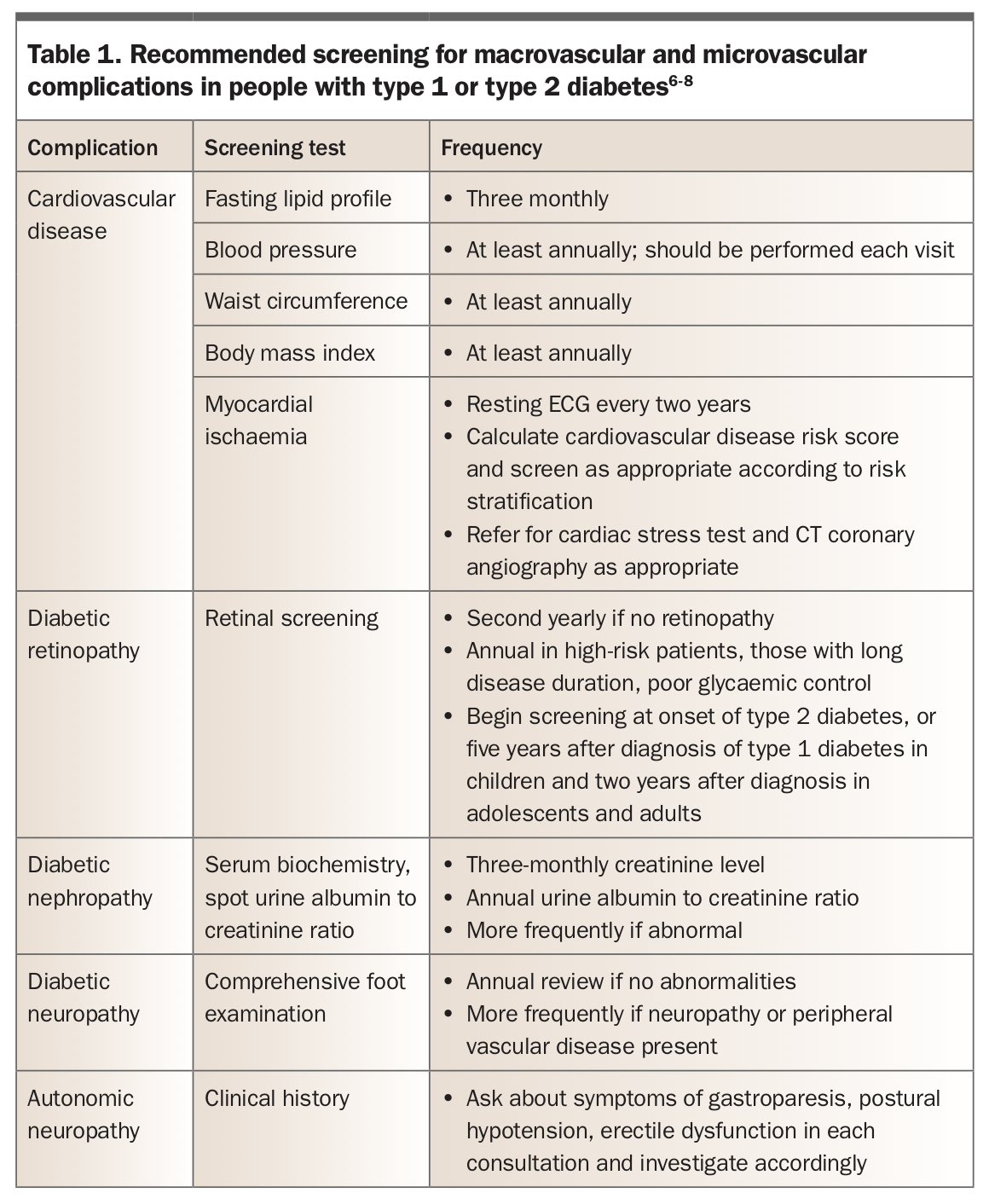
The current recommendations for screening for complications in people with diabetes are listed in Table 1.6,7,8 In addition to screening for microvascular and macrovascular complications, it is recommended that people with type 1 diabetes undergo screening for other autoimmune diseases. Patients with type 1 diabetes have higher risks of associated autoimmune conditions, such as coeliac disease and thyroid disorders.6 It is recommended that patients with type 1 diabetes have thyroid stimulating hormone (TSH) level measured annually and that screening for coeliac disease be considered.6 The targets for glycaemic control and other risk factor modification are summarised in Table 2.8
{kind=link}
{kind=link}
Assessment for microvascular complications
Diabetic retinopathy
Adults with diabetes, regardless of type, should have an annual dilated eye examination to screen for diabetic retinopathy. Retinopathy can be asymptomatic in the early stages, but can progress rapidly; thus it is important to emphasise to patients that regular screening is essential. It is uncommon for patients with type 1 diabetes to develop retinopathy in the first three to five years of their disease; however, most will develop the condition at some point over the next 20 years.9 Up to 20% of patients with type 2 diabetes have retinopathy at the time of diagnosis, and many develop it over time.9
Diabetic retinopathy can be classified as proliferative or nonproliferative. Proliferative diabetic retinopathy is characterised by the presence of new blood vessels within the retina. Due to the increased vascularisation, they are prone to haemorrhage, which can lead to acute visual loss. In nonproliferative diabetic retinopathy, microaneurysms form in the early stage of the disease. Hard exudates can occur later in the disease and are prone to haemorrhage.7 Management of diabetic retinopathy often requires input from an optometrist, ophthalmologist, the GP and an endocrinologist. Current guidelines recommend frequent monitoring (between three- to six-monthly or annually, based on severity) for nonproliferative diabetic retinopathy. All patients with proliferative diabetic retinopathy or diabetic macular oedema should be referred for ophthalmology review on an urgent basis.7
Early identification of diabetic retinopathy allows an opportunity to slow progression with improved glycaemic control and control of other risk factors such as hypertension.9 The Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study provided evidence supporting a role for fenofibrate in patients with type 2 diabetes in reducing the need for laser therapy for diabetic retinopathy, independent of lipid levels.10 Early detection also allows earlier access to treatment that can reduce the risk of visual loss and need for vitrectomy, such as laser treatment, or intravitreal pharmacotherapy with a corticosteroid or anti-vascular endothelial growth factor.9
Diabetic nephropathy
Diabetes remains the leading cause of chronic kidney disease worldwide.11 All patients with diabetes should be screened annually for diabetic kidney disease. This develops in up to 20 to 40% of patients with type 1 or type 2 diabetes.11 General principles for slowing the progression of kidney disease include tight glycaemic control, along with treatment with an ACE inhibitor or an angiotensin receptor blocker, if there are no contraindications.11 Sodium-glucose cotransporter-2 (SGLT-2) inhibitors also have a role in preventing progression of chronic kidney disease in patients with type 2 diabetes and existing microalbuminuria and mild renal impairment.12,13 Glucagon-like peptide-1 (GLP-1) agonists have also been shown to reduce the rate of development and progression of diabetic nephropathy in people with type 2 diabetes.14
The presence of microalbuminuria is an early sign of diabetic nephropathy. If an initial test on a spot urine sample to determine the albumin to creatinine ratio does not show microalbuminuria, the patient should be retested annually. A single elevated spot urine albumin to creatinine ratio alone is not diagnostic and the test should be repeated several times over six months.8 Other causes of proteinuria, such as urinary tract infection, should be considered. The normal reference range for a spot urine albumin to creatinine ratio is less than 2.5 mg/mmol in men and less than 3.5 mg/mmol in women. A 24-hour urine collection can be used to further quantify the degree of proteinuria.
Serum creatinine level and estimated glomerular filtration rate (eGFR) should be monitored at least annually. A decline in eGFR to less than 60 mL/min/1.73m2 is abnormal. If this occurs, repeat testing within three months can be done to confirm whether this is transient.8
Diabetic neuropathy
Diabetic neuropathy is common, affecting up to 90% of patients with type 1 or type 2 diabetes;8 and diabetes is the leading cause of peripheral neuropathy. Symptoms can vary significantly between individuals, and some individuals have seemingly asymptomatic neuropathy. Some patients can experience painful feet and increased sensitivity, whereas others have reduced sensation, typically in a ‘glove and stocking’ distribution.15 Once present, neuropathy is irreversible, although improved glycaemic control can help to delay progression.5
A formal foot examination should be conducted annually, by either an experienced medical practitioner or a podiatrist. This involves checking for the presence of pedal pulses, testing sensation via monofilament testing and assessing proprioception and vibration. The general appearance of the foot should be noted, such as loss of hair over the distal shin, as these changes frequently reflect underlying microvascular disease. Close inspection of the feet for the presence of diabetic foot ulcers is important. Cracked skin on the dorsum of the foot may predispose a person to skin breakdown and infection, and should be closely inspected. Patients with identified diabetic neuropathy should have formal podiatry assessments on a three-monthly basis, or more regularly if clinically indicated.
A diagnosis of peripheral neuropathy can usually be made based on clinical features. However, nerve conduction studies can help confirm the diagnosis of diabetic neuropathy if the clinical picture is not clear.
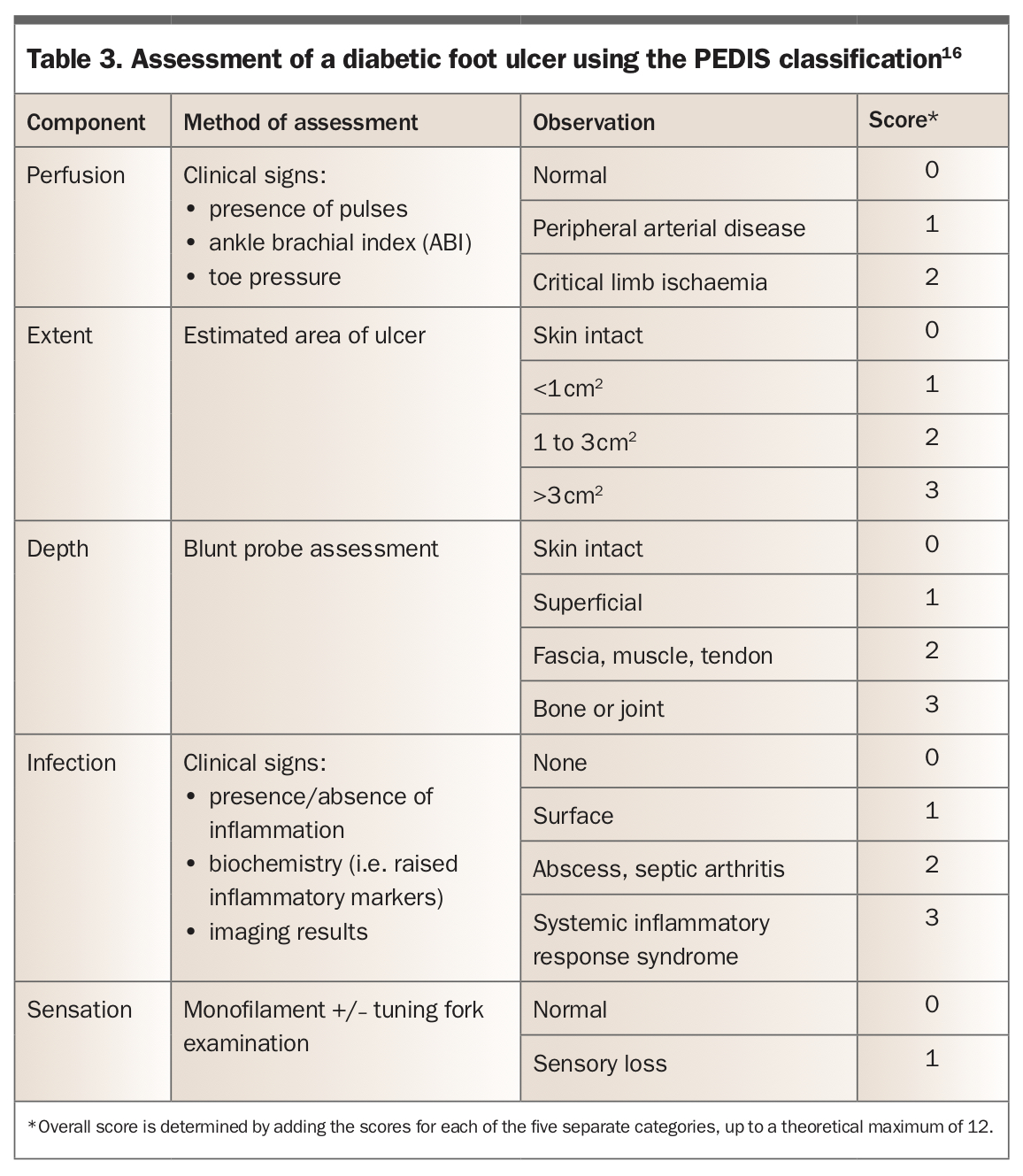
The presence of a diabetic foot ulcer should prompt assessment of clinical severity using tools such as the PEDIS (perfusion, extent, depth, infection, sensation) classification (Table 3).16 Patients whose feet show prolonged capillary refill (over 3 seconds) and are difficult to palpate or lack pedal pulses should undergo arterial doppler ultrasonography. Patients with nonhealing foot ulcers (over 4 weeks) should be referred to a multidisciplinary high-risk foot service.16
{kind=link}
Autonomic neuropathy is often under-recognised in people with diabetes, particularly those with type 1 diabetes. It may manifest as gastroparesis, erectile dysfunction or cardiac autonomic neuropathy. Its presence is associated with longer disease duration and poorer glycaemic control. Gastroparesis is characterised by delayed gastric emptying and can lead to feeling full quickly after eating, with or without reflux and abdominal pain. It can be formally diagnosed by a gastric emptying study. Erectile dysfunction in men with diabetes is common and requires careful evaluation. Cardiac autonomic neuropathy is likely underdiagnosed and has a significant impact on the risk of myocardial ischaemia, heart failure, arrhythmias and orthostatic hypotension. Changes in heart rate variability and blood pressure on sitting to standing can indicate cardiac autonomic neuropathy and require further evaluation.17
Assessment for macrovascular complications
Coronary artery disease
A large proportion of morbidity and mortality from diabetes is attributable to coronary artery disease. Although it is acknowledged that diabetes is a key risk factor for developing coronary artery disease, the question of knowing who to screen, when to start screening and how to screen is often a challenge for clinicians.
The Australian cardiovascular disease risk calculator developed by the National Heart Foundation of Australia is a tool for estimating the risk of heart attack or stroke within the next five years in older patients without a known history of cardiovascular disease or other comorbidities. Patients are stratified into low risk (less than 10% chance of an event within five years), moderate risk (10 to 15%) or high risk (over 15%).18 Factors taken into account when determining risk include age, diabetes, smoking status and family history of cardiovascular disease.
All patients with diabetes aged over 60 years or with diabetes and microalbuminuria are considered high risk. Aggressive cardiovascular risk factor modification is generally recommended in such patients.18 Antihypertensive therapy is strongly recommended for patients with diabetes who have hypertension (systolic blood pressure over 140 mmHg).8 Renin-angiotensin system blockade is generally the preferred treatment, owing to its renoprotective effects. More recent data have shown a role for finerenone, a mineralocorticoid receptor antagonist, in reducing risk of progression of chronic kidney disease in patients with type 2 diabetes.19
Lipid profile should be assessed regularly to help prevent macrovascular disease complications, and lipid-lowering therapy is recommended in all patients with diabetes and previous cardiovascular disease.8 Statins are generally first-line lipid-lowering therapy. Fenofibrate should be considered as an adjunct in patients with known diabetic retinopathy. Proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors can have a role in lowering LDL-cholesterol levels in patients who have not achieved the target range despite maximal-dose statin therapy.8 Patients with a history of diabetes and prior cardiovascular disease or a history of ischaemic stroke should be considered for antiplatelet therapy.18
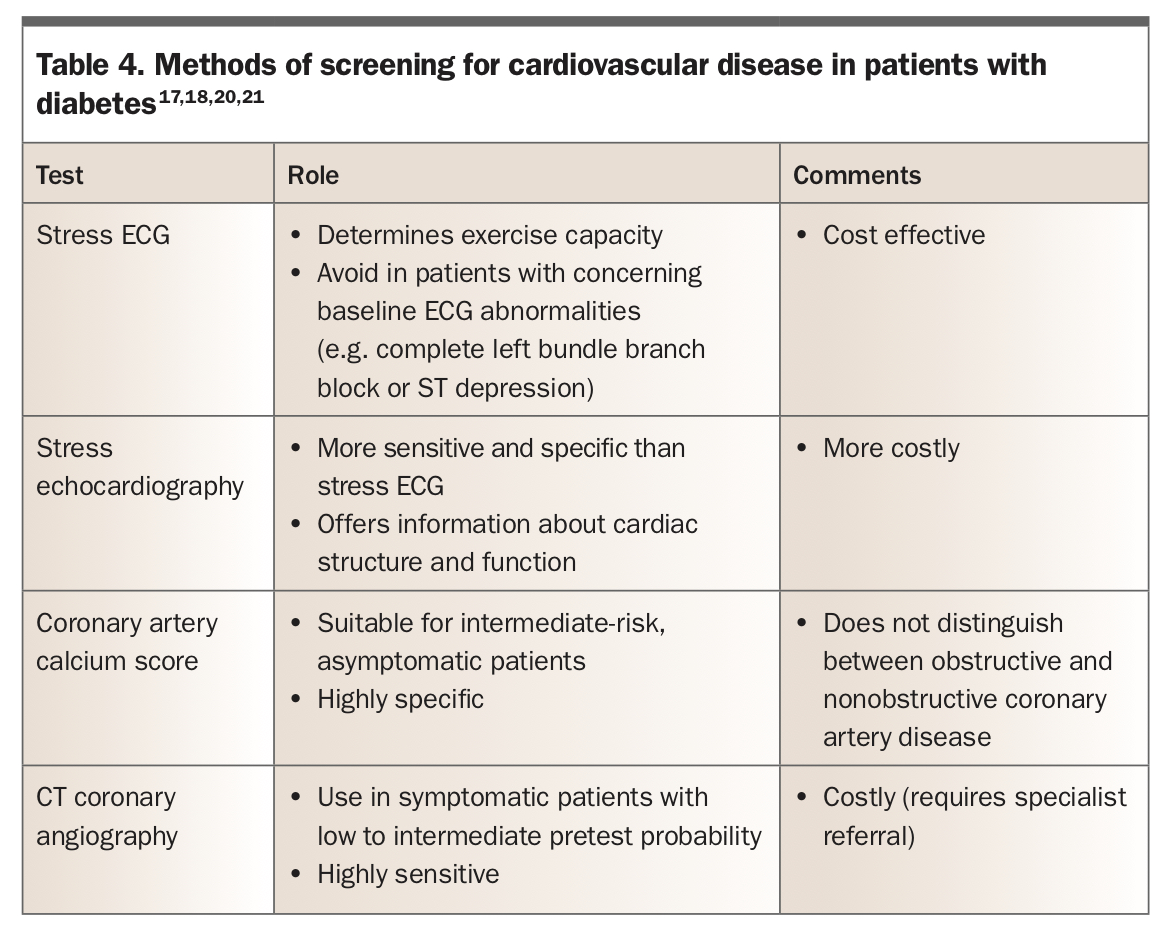
Patients with diabetes should have regular assessment of their cardiovascular risk profile. Low-risk patients should be reassessed every two years, moderate-risk patients every six to 12 months and high-risk patients as clinically indicated. Cardiac stress testing is valuable to assess patients with an intermediate pretest probability of coronary artery disease and is useful to further substratify patients into low or high risk.20,21 Methods of screening for cardiovascular disease are outlined in Table 4.17,18,20,21
{kind=link}
A positive stress ECG or echocardiogram should prompt a cardiology referral for consideration of CT coronary angiography.20 All patients should have counselling about further modifiable risk factors, such as smoking, alcohol intake, diet and physical inactivity. There are no current guidelines outlining whether to screen for heart failure in patients with diabetes. Routine clinical examination should assess for signs of cardiac failure, and if detected, a transthoracic echocardiogram should be arranged. SGLT-2 inhibitors can be a useful therapeutic option if heart failure is detected, as they have been found to reduce risk of hospitalisation or cardiovascular death in patients with heart failure with reduced ejection fraction and heart failure with preserved ejection fraction.22,23
Peripheral vascular disease
Diabetes is a major risk factor for the development of peripheral vascular disease (PVD). The presence of PVD is a major risk factor for lower limb amputation.16 Once PVD is diagnosed, thorough investigations for other forms of macro- and microvascular disease are essential.
The detailed foot examination previously outlined provides screening for the presence of PVD. The feet should be closely inspected for any evidence of ischaemia, noting the colour of the foot (in particular toe pallor or duskiness), temperature, pulses, and presence of pain, paraesthesia or paralysis.16 Patients should be asked about claudication symptoms at each visit. Tests such as ankle brachial index and lower limb doppler ultrasound should be considered, as described above.
Cerebrovascular disease
Although cerebrovascular disease is an important diabetes-related complication, there is no universal guidance regarding screening. Aggressive modification of cardiovascular risk factors can help reduce cerebrovascular risk.8 It is good practice to auscultate for the presence of carotid bruits on routine physical examination. If these are present, carotid artery doppler ultrasound should be arranged to look for the presence of carotid artery stenosis, which may increase cerebrovascular risk.
Other complications
Patients with type 1 or type 2 diabetes are at increased risk of cognitive decline, particularly with regard to deficits in attention, executive functioning, processing and memory.24 The Mini Mental State Examination (MMSE) can be a useful tool in screening for cognitive impairment.
The incidence of obstructive sleep apnoea is increased in patients with type 2 diabetes. Sleep studies should be considered in patients with risk factors for and symptoms of sleep apnoea.
Nonalcoholic fatty liver disease is strongly associated with type 2 diabetes, with insulin resistance being a key pathogenic mechanism. There are no clear guidelines for screening; however, the diagnosis should be considered in those with otherwise unexplained raised transaminase levels. Liver ultrasound can help further evaluation.
Further screening in specialised populations
Complications in pregnancy
Women with type 1 or type 2 diabetes need close monitoring by a specialist diabetes management team during pregnancy. In addition to standard pregnancy care, the HbA1c level should be monitored every two to three months.25 At the beginning of pregnancy appropriate baseline investigations include TSH, serum creatinine and HbA1c levels, lipid profile, eGFR and spot urine albumin to creatinine ratio. Women with type 1 diabetes should also have tests for thyroid autoantibodies, coeliac serology and vitamin B12 and red cell folate levels. Retinal screening should be performed in the first trimester. If retinopathy is present, it should be closely monitored throughout the pregnancy. If retinopathy is not present on initial screening, testing can be repeated in the third trimester. Measurement of a spot urine albumin to creatinine ratio should be repeated each trimester.25
Autoimmune conditions associated with type 1 diabetes
Type 1 diabetes can be associated with other autoimmune diseases, typically thyroid disease, coeliac disease, pernicious anaemia and vitiligo.26 Addison’s disease, although less common, is an important coexisting disease to exclude and should be considered if patients develop frequent, unexplained hypoglycaemia. Autoimmune polyendocrine syndromes should be considered in those with type 1 diabetes and coexisting hypoadrenalism.
Thyroid disease is the most prevalent coexisting autoimmune disease in patients with type 1 diabetes. At diagnosis of type 1 diabetes, thyroid function (TSH, free thyroxine, tri-iodothyronine), antithyroid peroxidase antibodies and antithyroglobulin antibodies should be measured. About eight to 15% of young people with diabetes test positive for thyroid peroxidase antibodies at diagnosis.26 Annual thyroid function tests are generally recommended; however, this may be stretched to two yearly in patients with negative thyroid antibody test results. A combination of TSH and thyroid autoantibody tests can be used for annual screening in those with an initial positive thyroid autoantibody test result.6
Coeliac disease is more common in patients with coexisting type 1 diabetes. It can be asymptomatic but has important implications for nutrition and glycaemic management due to altered gastrointestinal absorption. Patients who are younger at diagnosis of type 1 diabetes have an increased risk. Screening is by measurement of IgA and antitissue transglutaminase antibody levels. When there are equivocal test results and high clinical suspicion, the patient should be referred to a gastroenterologist for consideration of endoscopy and biopsy.26 There is no clear consensus for the frequency of screening for coeliac disease; however, the International Society for Paediatric and Adolescent Diabetes (ISPAD) recommends screening at diagnosis for children with type 1 diabetes, with repeat annual screening for the first five years and two-yearly thereafter.6
In people with type 1 diabetes, pernicious anaemia is screened for by measuring vitamin B12 levels; however, there is no current recommendation on frequency. Patients taking metformin also need to have vitamin B12 levels monitored, as metformin has been shown to lower vitamin B12 absorption in the gastrointestinal tract.
Conclusion
Diabetes is a common disease with a range of potential micro- and macrovascular complications that can be a significant health burden for individuals and the broader healthcare system. Careful screening for the development of these complications can allow earlier detection, which can provide the opportunity to implement preventive measures that may halt progression. Good glycaemic control is pivotal in helping reduce risk of complications. ET
COMPETING INTERESTS: Dr White: None. Dr Glastras has received consulting fees from Novo Nordisk and Sanofi; payment for presentations, speaker bureaus, manuscript writing and educational events from Novo Nordisk, Sanofi, Boehringer Ingelheim, Eli Lilly, Medtronic and Roche; and support for attending meetings and travel from Novo Nordisk.