Androgen replacement in men. Maximising efficacy, minimising adverse effects

Endocrine diseases
Men's health
It is vital to establish a definitive diagnosis of hypogonadism before starting testosterone replacement therapy, as the treatment is lifelong. Maximal efficacy with minimal adverse effects is achieved through individually tailored treatment and thorough monitoring after treatment initiation.
- In men with hypogonadism, testosterone deficiency is a clinical diagnosis confirmed by hormone assays.
- A definitive clinical diagnosis (including testicular examination) needs to be made before starting testosterone treatment.
- There is no role for a ‘trial’ of testosterone replacement therapy (TRT).
- There is no evidence of benefit from TRT in testosterone deficiency resulting from chronic disease, ageing or obesity.
- TRT needs to be initiated by or in consultation with a specialist.
- The best way of maximising the benefit and minimising the risk of TRT is to treat only men for whom the benefit is proven; that is, those with properly established androgen deficiency due to pathological hypogonadism.
Androgens (from the Greek ‘andros’, meaning ‘man’) are steroid hormones responsible for the development and maintenance of male sexual characteristics that exert their effects through androgen receptors.1 Testosterone is the main androgen, others being androstenedione (the precursor to testosterone) and dihydrotestosterone.
Androgen deficiency is a feature of hypogonadism, which is a pathological disorder of the reproductive system. This is a clinical diagnosis confirmed by hormone assays. Testosterone is used clinically at physiological doses as androgen replacement therapy in men with pathological hypogonadism. The principal goal of treatment is to restore the physiological level of androgen exposure in tissues so it is similar to that in eugonadal men.1
Aetiology of hypogonadism
The testes have two physiological functions: spermatogenesis and steroidogenesis, and any impairment in these pathways leads to infertility and androgen deficiency. Leydig cells, which secrete testosterone, are more robust than the sperm-producing germinal epithelium, so androgen deficiency is unlikely in the presence of normal spermatogenesis whereas most men with impaired spermatogenesis are not androgen deficient. Testosterone production is regulated by a tight negative feedback from the hypothalamic-pituitary-testicular (HPT) axis.
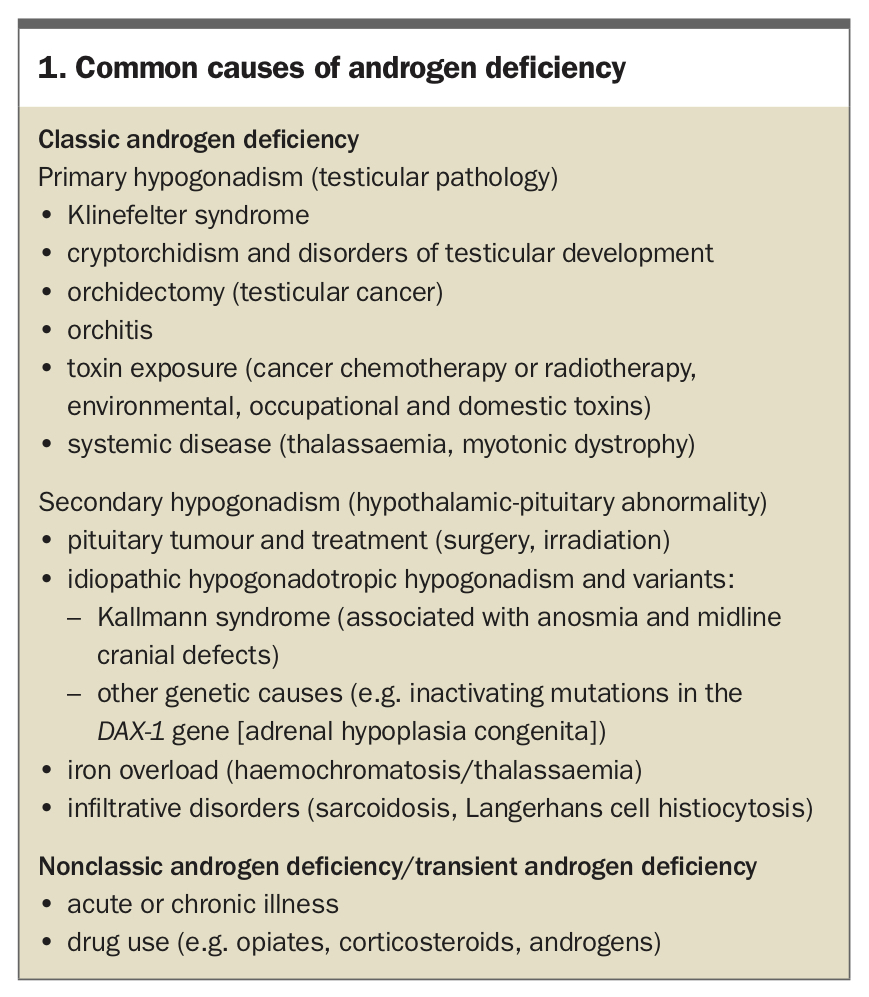
It is important to establish the aetiology to guide management of hypogonadism. The broad classification of classic androgen deficiency includes:
- primary hypogonadism from a testicular cause
- secondary hypogonadism due to a pituitary or hypothalamic cause.
Transient or partial androgen deficiency can occur in acute or chronic disease states or owing to the use of drugs, such as opiates, androgens for body building, or corticosteroids. In these circumstances, resolution of the underlying condition or cessation of the drug use leads to recovery of the HPT axis. The recovery can be slow and prolonged in cases of androgen abuse, taking between nine to 18 months after stopping the drug use, but is eventually complete.2 Serum testosterone level may be low in men with intercurrent illness or chronic disease (obesity, excessive alcohol intake), but this does not generally require treatment. The prevalence of classic androgen deficiency is about one in 200 adult men. Klinefelter syndrome remains underdiagnosed and is detected in only 10 to 30% of men with the condition during their lifetime.3,4 The common causes of androgen deficiency are listed in Box 1.
{kind=link}
Assessment for hypogonadism
Androgen deficiency is a clinical diagnosis, confirmed by laboratory hormone assays.5 The symptoms are nonspecific unless the patient is severely androgen deficient, and a careful evaluation should be undertaken.
A complete evaluation includes a thorough history and examination. Signs and symptoms of androgen deficiency depend on the age at presentation. During fetal life, at birth and in the neonatal period, androgen deficiency leads to disorders of sexual differentiation (ambiguous genitalia, cryptorchidism, micropenis, etc). During adolescence, androgen deficiency can present as delayed puberty. In adulthood, androgen deficiency causes hormone deficiency symptoms and regression of some features of virilisation.6 History should include childhood, pubertal and fertility history and symptoms of androgen deficiency, which can be nonspecific, such as reduced energy levels, lethargy, easy fatiguability, decreased endurance capacity and reduced libido. Flushing is rare in mild to moderate deficiency and is usually only experienced in men with castrate testosterone levels.
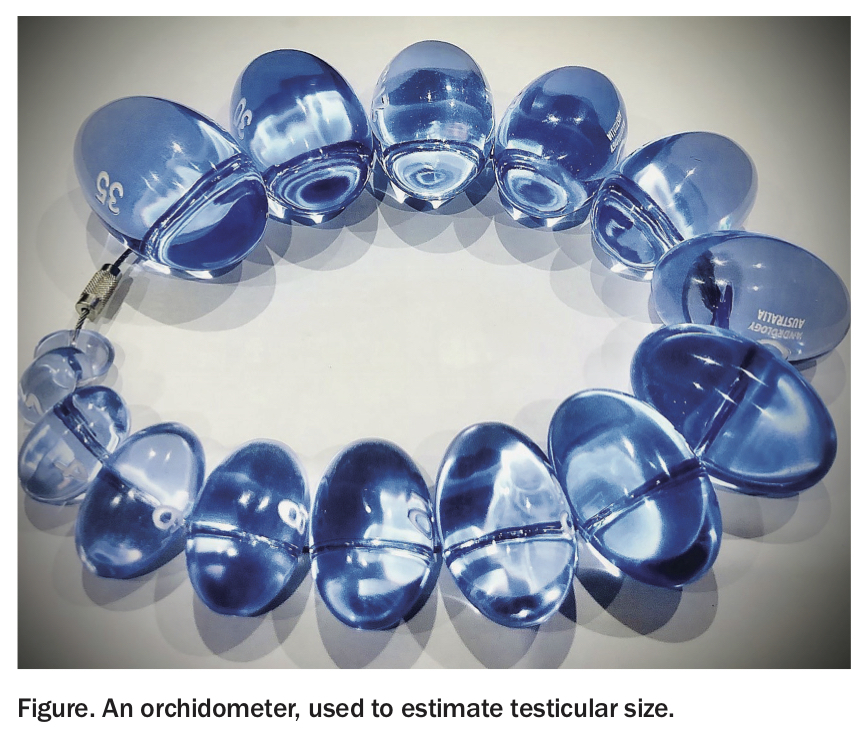
Testicular examination is a vital part of physical examination along with a complete general examination. Examination should be undertaken in a warm room, with the patient lying on his back. The examiner gently isolates the testis, stretching the scrotal skin, without causing any compression of the testis. The orchidometer bead (Figure 1) estimated to be closest to the size of the testis is then held next to the testis to make a side-by-side comparison. Size of the testis is a good indicator of its function and a normal testis should feel firm. The presence of normal testicular size excludes androgen deficiency unless of very recent onset. Other features to look for include gynaecomastia, loss of body hair and decreased muscle bulk.
{kind=link}
Investigations help confirm the clinical diagnosis, and most causes are established by measuring total testosterone, sex hormone binding globulin (SHBG), luteinising hormone (LH) and follicle stimulating hormone (FSH) levels in a morning serum sample.5 Most of the testosterone is bound to SHBG, and SHBG levels should be considered when interpreting serum testosterone results, as a low SHBG level results in a falsely low testosterone level and vice versa. Terms such as ‘free’, ‘calculated free’ and ‘bioavailable’ are often reported. They are not validated and do not have practical clinical application.7 Primary hypogonadism results in low testosterone with high gonadotropins (LH and FSH) and secondary hypogonadism results in low testosterone with low or normal gonadotropins. Serum prolactin level, iron studies, karyotype and pituitary imaging should be considered to further establish the aetiology of hypogonadism.
Obesity is commonly associated with a low testosterone level, low SHBG level and normal LH and FSH levels. It is not an androgen deficient state and is reversed by weight loss. Obesity alone is not an indication for testosterone replacement therapy (TRT).8
Management of androgen deficiency
It is vital to establish a definitive diagnosis before starting TRT, as the treatment is lifelong. Contraindications include untreated prostate and breast cancer. Men over 50 years of age should undergo a baseline prostate-specific antigen (PSA) test before initiating treatment, and a digital rectal examination could be considered. In patients in whom testosterone is low due to intercurrent illness or chronic systemic disease, treatment should be aimed at treating the underlying condition as TRT is unlikely to be beneficial. A short course or trial of TRT would only prolong the diagnostic dilemma and should be avoided. Recovery of HPT axis suppression caused by such treatment can be very prolonged after cessation of TRT.2 Testosterone treatment should not be initiated in men seeking fertility in the short term.9 Sperm banking should be considered if they are not azoospermic and require TRT.
In men with delayed puberty, testosterone treatment helps development of secondary sexual characteristics.10 In hypogonadal men, treatment is beneficial for sexual function (libido, erection and sexual activity).11 Testosterone treatment in men with pathological hypogonadism improves volumetric bone mineral density and bone strength.12 Testosterone should not be used as monotherapy in osteoporosis or in men with increased fracture risk.9
Treatment aims are to restore and maintain physiological tissue androgen exposure and replicate eugonadal blood testosterone levels, and to maintain ongoing compliance. Treatment should begin at full dose except in older men or those with delayed puberty. Long-term compliance depends on a convenient and acceptable regimen and the accessibility of therapy options. Prescribing of testosterone under PBS authority is tightly regulated by the following conditions.5
- Men who have classic androgen deficiency due to hypothalamic-pituitary or testicular disorders: must be treated by, be in consultation with or have an appointment to be assessed by an appropriate specialist (general paediatrician, paediatric endocrinologist, endocrinologist, urologist or sexual health medicine specialist). This is restricted to initiation of treatment by a specialist for men with classic androgen deficiency.
- Men who do not have classic androgen deficiency (no established pituitary or testicular disorders), but who are 40 years of age or older and androgen deficiency is not due to age, obesity, cardiovascular disease, infertility or drugs: at least two morning blood samples should be taken on different mornings. Androgen treatment is allowed under the PBS if the testosterone level is less than 6 nmol/L, or 6 to 15 nmol/L with a high LH level (>1.5 times the upper limit of the eugonadal reference range for young men or >14 IU/L). Treatment must be initiated by a specialist, as for classic androgen deficiency. The above conditions for men who do not have classic androgen deficiency are arbitrary guidelines and there is no evidence for a benefit of TRT in such a scenario. Treatment may lead to testosterone dependence.
- Boys under 18 years of age with micropenis, constitutional delay of growth or puberty or who require pubertal induction: must be treated by, or in consultation with, or have an appointment to be assessed by an appropriate specialist (as above).
In Australia, testosterone can be administered topically as a gel, cream or patch and by intramuscular injections. There is no satisfactory oral preparation, due to side effects.
Transdermal testosterone preparations that are applied daily are available as a 1% (50 mg/5 g) gel in a sachet; 1% (12.5 mg/actuation) or 2% (23 mg/actuation) gel in a metered-dose pump; a 5% (50 mg/mL) cream; and patches (2.5 mg and 5 mg/24 hours). They are to be applied on clean, intact skin immediately after a shower. Topical applications are useful in people with bleeding disorders or when deep intramuscular injections are contraindicated. Use of the gel and cream carries the risk of transfer to close contacts. Patches frequently cause skin irritation from absorption enhancers.
Deep intramuscular injections are available as testosterone mixed esters 250 mg in 1 mL oil vehicle, administered usually every 3 weeks; testosterone enantate 250 mg in 1 mL oil vehicle, administered every two weeks; and testosterone undecanoate (TU) 1000 mg in 4 mL oil vehicle, which is administered about every 12 weeks. TU requires a loading dose at six weeks after initiating therapy. The long-acting TU has the advantage of convenience, with four injections a year, and is convenient in most clinical settings. Contraindications include bleeding disorders.
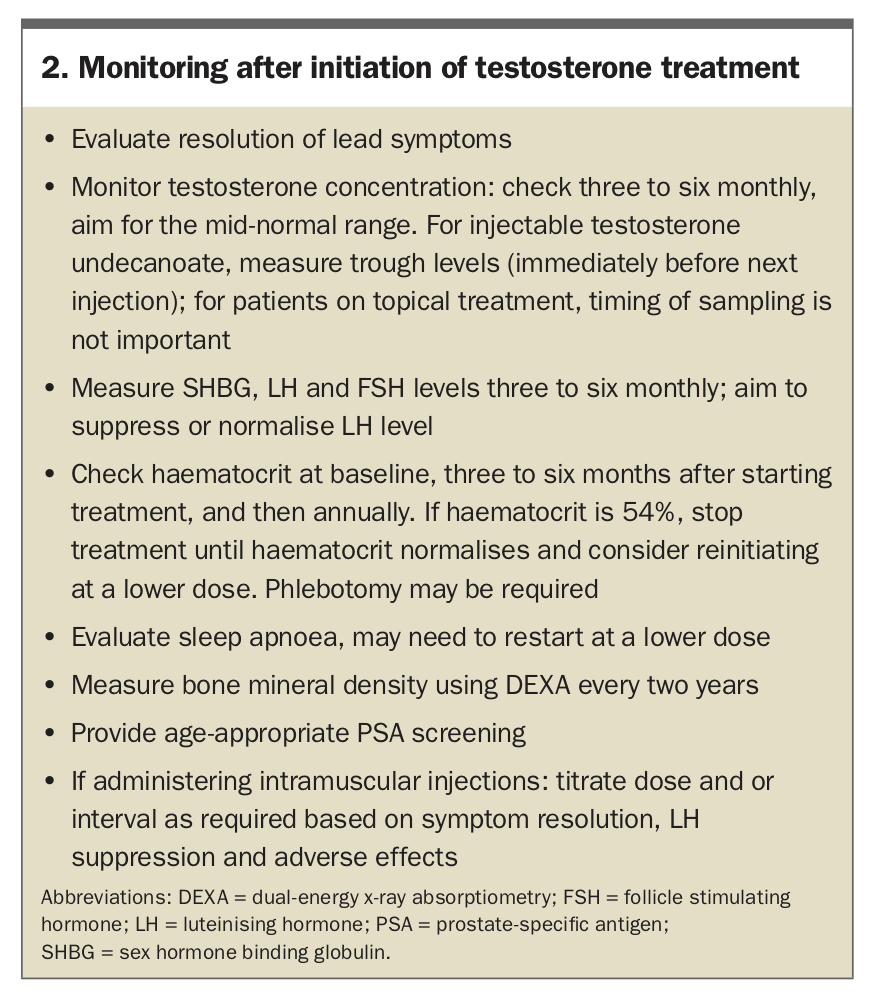
The aspects of monitoring involved after initiating treatment are summarised in Box 2. The best clinical measure of adequate treatment is the resolution of the man’s leading symptom.13 Monitoring should ensure normalisation of testosterone levels and, for primary hypogonadism, normalisation of LH level. Testosterone should be maintained in the mid normal range for healthy men.9 Testosterone treatment causes erythrocytosis (haematocrit >54%), an effect seen more in older men and smokers.14,15 In such men with raised haematocrit, treatment should be withheld until the haematocrit has normalised. Restarting at a lower dose or increasing the interval between injections can then be considered. Phlebotomy or venesection may be considered if the patient is deemed high risk for a thromboembolic event. The haematocrit should be measured at three to six months, and annually once stable.9 Screening is needed for side effects such as polycythaemia and sleep apnoea and for PSA level in older men. PSA screening should be undertaken as appropriate for age. In men over 40 years, an annual PSA test with digital rectal examination may be undertaken for prostate cancer screening. An increase in PSA level of 1.4 ng/mL above baseline, a PSA level greater than 4.0 ng/mL or an abnormal prostate on digital rectal examination warrant further review with a urologist.9 Bone density should be measured about every two years to ensure improvement in age-specific scores. Symptoms of androgen deficiency resolve within days to weeks of initiating testosterone treatment; persistent symptoms despite treatment are unlikely to be due to androgen deficiency.
{kind=link}
Conclusion
There are a variety of formulations available to treat androgen deficiency in men with pathological hypogonadism, and treatment can be individually tailored. We can achieve maximum efficacy and minimum adverse effects by treating only men with established androgen deficiency. Treatment should always be initiated by or in consultation with a specialist. There is no role for treatment trial. ET