Newer insulins in diabetes and their clinical utility

Diabetes type 1
Diabetes type 2
Over the past few years, four insulins have been listed on the PBS, providing more options to potentially optimise glycaemic control in patients with diabetes. These insulins are insulin glargine 300 units/mL, insulin degludec 70%/ insulin aspart 30%, ultra-fast-acting insulin aspart and insulin lispro 200 units/mL.
- Four insulins have in recent years been listed on the PBS, providing clinicians and patients with more options to potentially optimise glycaemic control.
- These insulins are insulin glargine 300 units/mL (Toujeo), insulin degludec 70%/insulin aspart 30% (Ryzodeg 70/30), ultra-fast-acting insulin aspart (Fiasp) and insulin lispro 200 units/mL (Humalog U200).
- Potential advantages of some of these insulins include lower rates of nocturnal hypoglycaemia and more flexibility in dosing times.
- Regardless of the insulin used, assessment of diet and physical activity are crucial for all patients with diabetes. Initiation or changes to the type and/or regimen of insulin should preferably occur in a multidisciplinary setting with input from medical specialists, diabetes educators and dietitians.
Insulin has long been a treatment backbone for patients with diabetes. In Australia, about 32% of patients with diabetes currently require insulin therapy.1 Insulin types are generally divided into those which are basal (or long acting), prandial (used at meals) or combinations of basal and prandial (premixed insulins and coformulations).
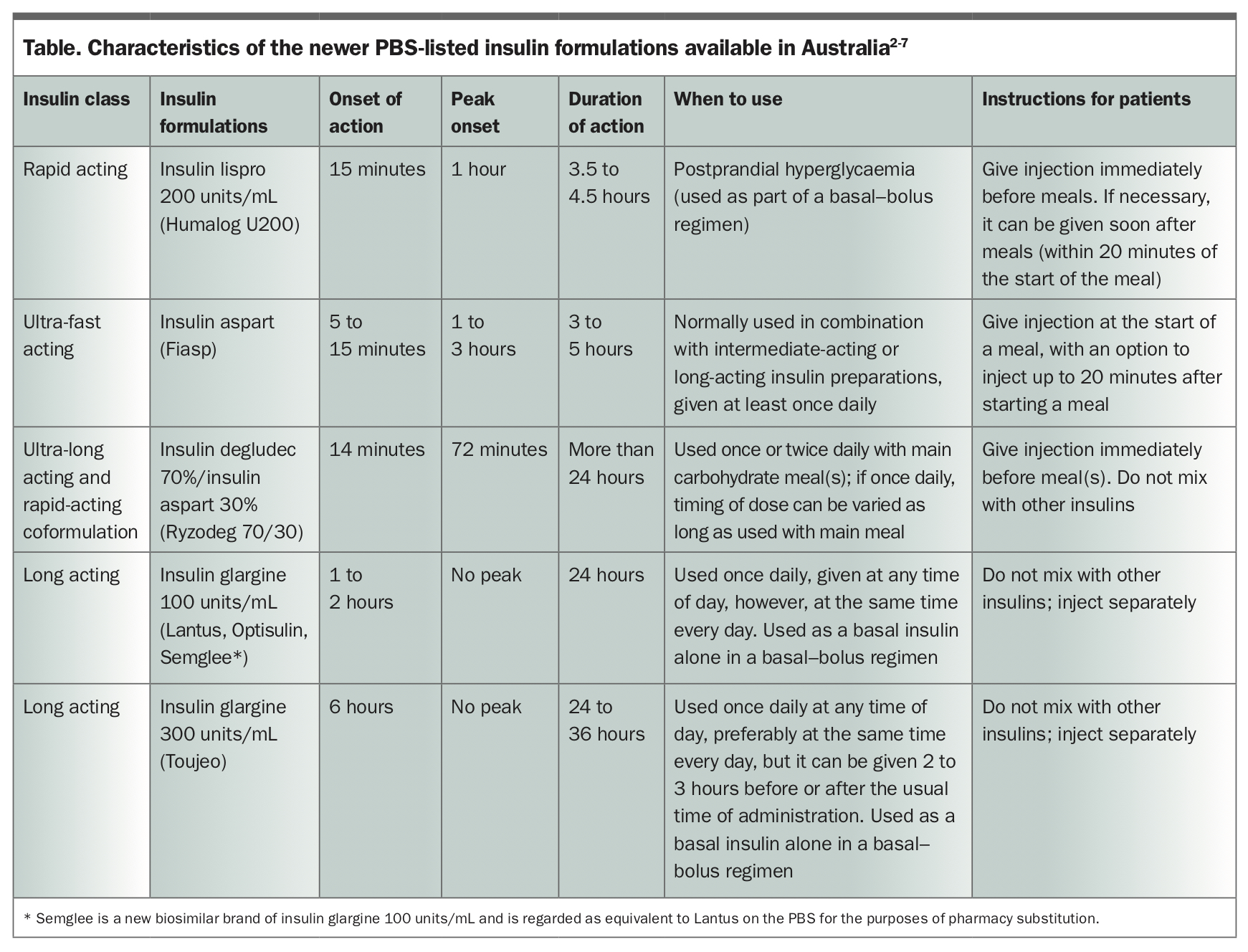
Over the past few years, four insulins have been listed on the PBS, providing clinicians and patients with more options to potentially optimise glycaemic control. These insulins are insulin glargine 300 units/mL (Toujeo), insulin degludec 70%/insulin aspart 30% (Ryzodeg 70/30), ultra-fast-acting insulin aspart (Fiasp) and insulin lispro 200 units/mL (Humalog U200). This article aims to provide an outline of the clinical utility of these insulin therapies. Key characteristics of these insulins are summarised in the Table, and each insulin delivery pen is shown in the Figure.2-7
{kind=link}
Insulin glargine
Since 2006, insulin glargine 100 units/mL (Lantus) has been available on the PBS for use in patients with type 1 or type 2 diabetes. It has been the most frequently used basal insulin therapy in Australia. From 1 July 2020, the brand Lantus will no longer be marketed, but will be replaced by the brand Optisulin (identical to Lantus but with different packaging, also using the SoloStar delivery device but with a variation to the colour of the pen). Also, Semglee is a new biosimilar brand of insulin glargine 100 units/mL and is regarded as equivalent on the PBS to Lantus for the purposes of pharmacy substitution. Semglee has been assessed by the TGA on the basis of comparability and clinical studies to be highly similar to Lantus.
In April 2018, insulin glargine 300 units/mL (Toujeo) was listed on the PBS for the same indication as insulin glargine 100 units/mL. Insulin glargine 300 units/mL is a more concentrated formulation and is an option for patients who have been prescribed high doses of insulin or are taking insulin glargine 100 units/mL twice daily, as a lesser volume of insulin is injected subcutaneously for an equivalent dosage. The lesser volume may reduce discomfort experienced from large-volume administration and may be easier to administer because of less ‘dialling up’ of the pen to administer the required dose.
Insulin glargine 300 units/mL has been shown in studies to be associated with a lower rate of nocturnal hypoglycaemia when compared with both insulin glargine 100 units/mL and insulin detemir 100 units/mL (Levemir).8 This is in part due to the delayed onset of action of insulin glargine 300 units/mL (over a period of six hours) compared with insulin glargine 100 units/mL (one hour), and its flatter profile and longer half-life (19 to 24 hours) combined with lower glycaemic variability.8 The timing of administration of insulin glargine 300 units/mL can also be relatively flexible in that it can be given two to three hours either side of the usual administration time with no disadvantage.
As insulin glargine 300 units/mL is dispensed using the SoloStar disposable pen (same as insulin glargine 100 units/mL), the transition is relatively seamless. Each SoloStar pen stores 450 units of insulin. Hence, it would also be a practical option for patients on stable insulin doses who have difficulty in accessing medical services or prescriptions regularly, such as those in rural or remote communities. Similarly, patients under financial strain may prefer insulin glargine 300 units/mL, as both insulin glargine formulations cost A$41 on the PBS but the cost per unit of insulin is less for insulin glargine 300 units/mL compared with insulin glargine 100 units/mL.
There are some cautions when switching to insulin glargine 300 units/mL, as a longer half-life means that patients potentially may remain above their blood glucose targets initially until a steady state concentration is achieved, up to a week after switching to insulin glargine 300 units/mL. Importantly, some studies indicate an approximate total daily dose increase of 15% may be required to achieve glycaemic control similar to that achieved using insulin glargine 100 units/mL.9,10
As with the use of other insulins, either in initiating or changing therapy, a consultation with the patient’s diabetes team is encouraged. It is also crucial that insulin glargine 300 units/mL should always be administered using the pen device provided and never with a syringe and, as such, it is not available in cartridge form. This is because of the inherent danger of potentially aspirating and injecting three times the appropriate amount of insulin because of the more concentrated form of this insulin.
Insulin degludec and insulin aspart
Insulin degludec 70%/insulin aspart 30% (Ryzodeg 70/30) is a coformulation of an ultra-long-acting basal insulin (insulin degludec) and rapid-acting insulin aspart in a ratio of 70:30. The properties of each individual insulin are maintained while in solution and also when injected. The insulin aspart component dissociates into the bloodstream rapidly just as insulin aspart does when injected on its own.
Insulin degludec has a half-life of 42 hours, greater than insulin glargine (24 hours) and insulin detemir (20 hours) with less intra- and interindividual variability. Insulin degludec has a flatter basal profile compared with other basal insulins and, once injected, forms a soluble multihexamer depot, which dissociates slowly.11 Insulin degludec is associated with lower overall hypoglycaemia and significantly lower rates of nocturnal hypoglycaemia compared with insulin glargine 100 units/mL, with equivalent glycated haemoglobin control.12 A single ingredient insulin degludec (Tresiba) has been recently TGA approved but is not yet subsidised on the PBS
Compared with traditional premixed insulins, insulin degludec and insulin aspart work independently of each other as a coformulation, both maintaining their distinct pharmacokinetic and pharmacodynamic properties. The insulin aspart works in the same way as any injection of insulin aspart would, while the insulin degludec functions individually as a basal insulin. As such, there is no ‘shoulder effect’ (interference between bolus and basal insulins) in contrast to that found when premixed insulins are used.13
Further, insulin degludec 70%/insulin aspart 30% has a lower rate of nocturnal hypoglycaemia compared with premixed insulins.14
Insulin degludec 70%/insulin aspart 30% is given before meals, once or twice daily, typically with the largest carbohydrate meal(s) of the day. If given twice daily, the doses should be administered six to eight hours apart from each other, typically at breakfast and dinner. Administration of the insulin does not require re-suspension. This enables ease of use compared with premixed insulins, where re-suspension is required with the potential for inadequate re-suspension and, thus, variable effects of the insulin.
The use of the coformulation of prandial and basal insulin may enable a decrease in the total daily number of insulin injections compared with a basal–bolus regimen. Insulin degludec 70%/insulin aspart 30% is an appealing option for patients who do not wish to take multiple subcutaneous injections but are open to once-daily injections with their main meal, for example, at dinner only, rather than injecting at dinner as well as before bedtime.
Timing of the injection can be varied by up to eight hours. Therefore, a patient may be able to administer insulin degludec 70%/insulin aspart 30% at breakfast on one day, for example on a weekday, and at lunch the next day, for example on the weekend. The carbohydrate intake has to be sufficient and appropriate for the insulin aspart component. This potential flexibility can be beneficial for patients who may forget to administer their insulin on occasion.
As with any prescription, clinical acumen is required when prescribing insulin degludec 70%/insulin aspart 30%, as the 70% basal to 30% bolus split may not be appropriate for all patients, and the combination may not be suitable for patients with large dietary variability. Dose adjustments are recommended only once every three to four days due to the long duration of action of insulin degludec, making titration difficult in some circumstances, such as during a hospital admission when changes to insulin doses may be necessary daily. In these situations, use of insulin glargine 100 units/mL or a premixed regimen may be more appropriate. Insulin degludec 70%/insulin aspart 30% is available in Australia using the FlexTouch pen. A feature of the pen is that it requires a lower injection force than other prefilled pens. See Table for newer insulin formulations.
{kind=link}
Ultra-fast-acting insulin aspart
An ultra-fast-acting insulin aspart (Fiasp) was listed on the PBS in June 2019. It differs from the commonly used insulin aspart due to the action of vitamin B3 in expediting insulin absorption, leading to an earlier onset of action (five minutes faster than insulin aspart [NovoRapid]).2 This may have significant clinical benefits in certain patient populations, including patients with type 1 diabetes who may not be certain of their meal quantity until after they start eating. Ultra-fast-acting insulin aspart would be advantageous in these circumstances as it can be administered up to 20 minutes after starting a meal, due to its rapid onset of action. Dose adjustments and blood glucose monitoring have to occur as with any insulin regimen, and in the case of ultra-fast-acting insulin aspart to prevent postmeal hypoglycaemia. Ultra-fast-acting insulin aspart would also be of clinical use in patients who forget to administer their prandial insulin five to 10 minutes before a meal, or in patients who are uncertain how much they will eat until they actually sit down to do so. The duration of action of ultra-fast-acting insulin aspart is similar to insulin aspart in pharmacokinetic–pharmacodynamic studies at 300 minutes, but there is more effect in the first 30 minutes following the injection. There are no consistent differences in glycated haemoglobin control when compared with insulin aspart. Ultra-fast-acting insulin aspart is dispensed using the FlexTouch pen.
In general, it is preferable that a change to ultra-fast-acting insulin aspart is only performed in conjunction with the patient’s diabetes team to ensure continuity of care. Caution must be taken for whom ultra-fast-acting insulin aspart is prescribed, as it may potentially increase the risk of hypoglycaemia in elderly or hypo-unaware patients.
Insulin lispro
Insulin lispro 200 units/mL (Humalog U200) was listed on the PBS in 2018, and is a more concentrated formulation of insulin lispro 100 units/mL (Humalog U100). Insulin lispro 200 units/mL may be useful particularly if large doses with less volume are required for each injection. It should always be administered using the KwikPen and not a syringe as otherwise there is a danger of administering twice the amount of insulin prescribed.
Conclusion
As the spectrum of oral hypoglycaemic agents expands, so do the available insulin therapies. There are potential advantages associated with these newer insulins, particularly relating to decreases in nocturnal hypoglycaemia in the case of insulin glargine 300 units/mL and insulin degludec 70%/insulin aspart 30% compared with insulin glargine 100 units/mL and premixed insulins, respectively, and improved patient adherence due to ease of dosing or flexibility in dosing times. The role of insulin glargine 300 units/mL, insulin degludec 70%/insulin aspart 30%, ultra-fast-acting insulin aspart and insulin lispro 200 units/mL may become more prominent as personalised, patient-focused therapies (rather than disease-focused therapies) come to the fore. Regardless of the insulin used, assessment of diet and physical activity are vital for all patients. Initiation or changes to the type and/or regimen of insulin is preferable in a multidisciplinary setting with medical, diabetes educator and dietitian input. ET
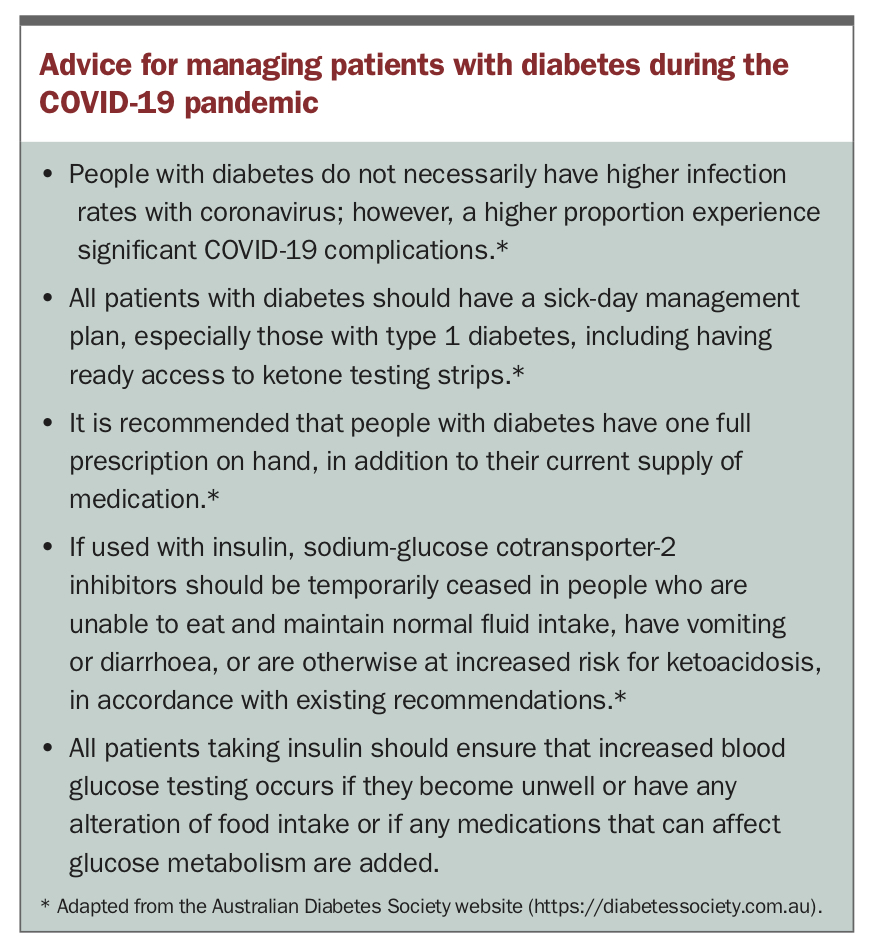
COVID-19 and diabetes
Advice from the authors of this article on managing patients with diabetes during the COVID-19 pandemic is provided in the Box.
{kind=link}
COMPETING INTERESTS: Dr Munsif: None. Associate Professor Chen has received speaker fees for educational meetings and is an adviser for Novo Nordisk, Sanofi, Eli Lilly, Boehringer Ingelheim, AstraZeneca and MSD.