Complementary medicines and diabetes: benefits, safety and risk

Diabetes medicines
Complementary and alternative medicine
People with diabetes often use complementary medicines (CMs) for a range of reasons. GPs have a responsibility to consider, ask about and document CM use as part of optimal diabetes care. The quality of the evidence to support CM use varies among studies. Personalised care and quality use of medicines are useful frameworks for making decisions about all types of medicines.
- Diabetes is an independent predictor of use of complementary medicines (CMs).
- People may not disclose use of CMs often because clinicians do not ask about it.
- Benefit, burden and risk apply to all medicines. People with diabetes assess these issues differently from clinicians and relate better to qualitative explanations than statistical information.
- The effects of CMs should be monitored and documented as part of the overall medicines regimen.
- Quality use of medicines, personalised care, shared decision-making and integrative medicine principles are useful frameworks to enhance benefit and safety and reduce risks of CM use.
Complementary medicine (CM) refers to a broad domain of healing resources that encompasses health systems, modalities, practices and their accompanying theories and beliefs that are not part of conventional medicine.1 Some 80% of the world’s population depends on CMs, which are often used within traditional medical systems.1 Specific CMs and systems differ among countries and cultures. Migration and refugee displacement through war and natural disasters mean the type of CM available outside people’s country of origin is increasing as they bring CMs to their new countries. These products may not be subject to the regulations and manufacturing and labelling standards that control many of the systems-related risks associated with medicine use.
Diabetes is an independent predictor of CM use.2 However, the prevalence of CM use in Australia ranges from 17 to 73%, depending on the age group and culture.2 People use CM to manage a range of conditions, including stress, pain, end-of-life care and blood glucose levels, often together with their conventional medicines, which puts them at risk of drug interactions and adverse events. Some CMs have a greater risk than others: some risks are theoretical and others are well documented. Many people self-prescribe CMs and more than 50% may not inform their GP about their CM use, often because the GP and other clinicians do not ask about it. Commonly used CMs include herbal medicines, vitamin and mineral supplements, probiotics, body therapies and mind-body therapies.3
Benefit, safety and risk
Benefit, safety and risk are complex interrelated issues rather than distinct concepts. Risk is part of everyday life. Individuals determine the level of risk they are willing to tolerate according to the perceived risk to them.4 Risk perceptions of people with diabetes differ from that of GPs. Many people in the general population and those with diabetes often underestimate their personal risk (optimistic bias).5,6 Previous experience, current health status, the media and health beliefs and attitudes influence personal risk perception. GPs and other clinicians often use statistical explanations to convey risk and benefit, which influences the emphasis they place on specific issues. People generally and those with diabetes often prefer, and may derive greater benefit in terms of health literacy and outcomes, less quantitative and more personalised direct explanations.5
GPs should conduct a thorough history and assessment to make a diagnosis, decide whether medicine(s) are required, their dose, dose interval, route and duration of use, and estimate potential risk and benefit for any management strategy. This includes asking about:
- allergies and adverse effects to previous CMs and conventional medicines
- current health status, particularly renal, liver and cardiac status
- smoking and alcohol use
- an up-to-date medicine list that includes CMs, self-prescribed medicines and other complementary therapies such as acupuncture and massage.
CMs and conventional medicines can cause adverse events. Both also have benefits if used within a quality use of medicines framework. A great deal of the evidence for CM safety is based on a long history of safe traditional use. However, modern extraction and manufacturing processes differ from traditional practices; therefore, some modern CMs are different from the original traditional preparations and may contain fewer or more active ingredients. There are three streams of approval: listed, registered and assessed. Assessed is a new pathway that involves the manufacturer supplying evidence for the efficacy of their products. The listed category only covers safety and good manufacturing practice.
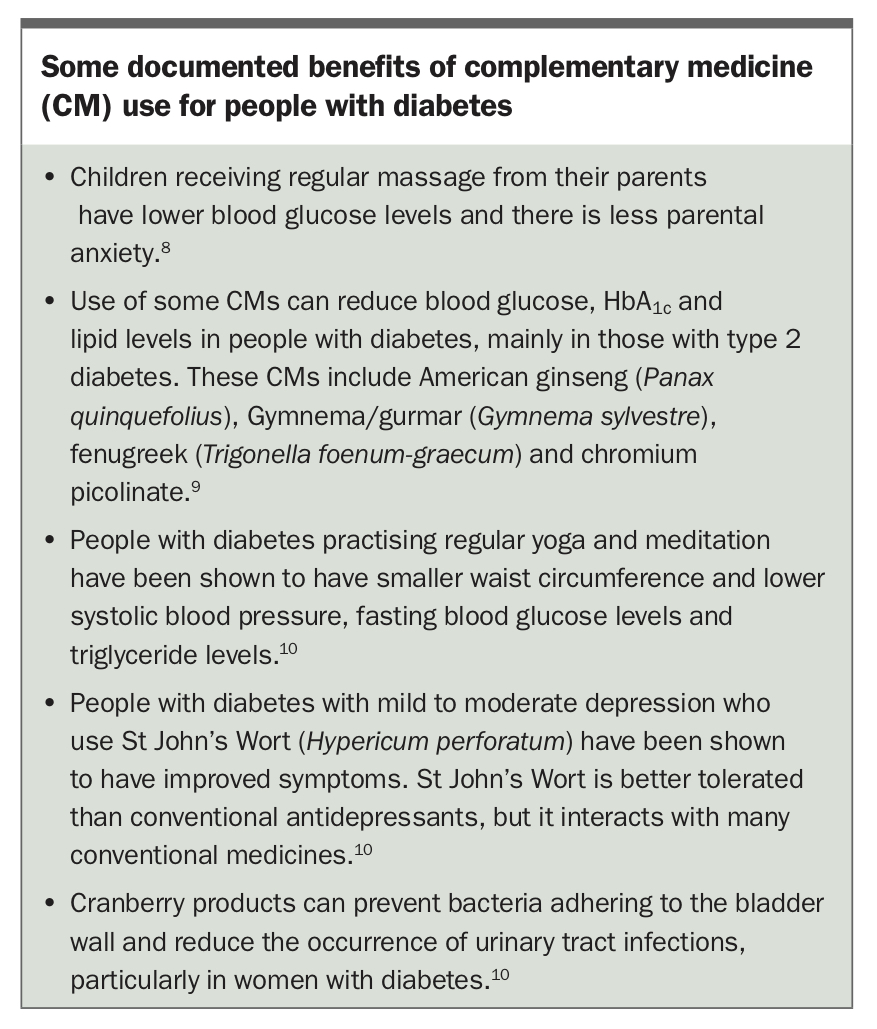
People often self-diagnose and self-treat, which can delay appropriate diagnosis and treatment and affect health outcomes. The safety and risk profile varies among CMs and the combination of CMs with conventional medicines (Table).7 In addition, CM use can contribute to polypharmacy and increase the overall medicine burden. Some documented benefits of CMs are shown in the Box.8-10
{kind=link}
Strategies GPs can use to improve safety and reduce risk
Quality use of medicines is a useful framework for determining treatment and assessing risk and can apply to conventional medicines and CMs. As indicated, regulatory processes are also important risk-management strategies. In Australia, CMs (herbal medicines, nutraceuticals, homeopathy and essential oils – but not raw herbs) are regulated by the TGA. Raw herbs are regulated under the Food Standards Australia New Zealand. GPs should, therefore, be particularly cautious when a person is using raw herbal products such as Chinese herbs and foods such as cinnamon. The NHMRC book Talking to Patients about Complementary Medicines can help GPs discuss CMs with their patients.11
Core components of quality use of medicines are outlined below.
- Select management options with the individual after undertaking a holistic assessment and considering relevant evidence, risks and benefits for the individual.
- Prescribe appropriately, including using medicines for prevention if indicated.
- Use medicines with lifestyle strategies to maximise their benefits. CM users are likely to use health promoting strategies and preventive health care.6
- Share decision-making with the individual, which includes providing people with objective, ethical information about all their care options, including CMs and other medicines/ therapies in a language and format they can understand.
- Monitor outcomes according to people’s reasons for using CMs in their healthcare plan (e.g. pain management), regularly updating a medicine list and reporting adverse events.
- Educate people with diabetes about safe CM use. Education for GPs could include how to read and critically analyse CM research findings and how to apply relevant findings in practice.
A concern is the training and competence of many CM practitioners. Many CM professional associations have stringent self-regulatory processes, including continuing professional development, but are not regulated under the Australian Health Practitioner Regulation Agency. This agency only regulates Chinese medicine, osteopath and chiropractic practitioners. Many CM practitioners are also concerned about inadequate training and the associated risks to patients. An increasing number of conventional practitioners prescribe CMs as part of integrative care.
Advice GPs can provide to help people with diabetes use CMs safely
It is imperative that GPs adopt a person-centred approach by genuinely listening, being open minded to the patient’s perspective and providing balanced advice in a nonjudgmental way that makes the patient feel listened to and validated, even if the GP advises them not to use CMs.
The following information could help GPs and people with diabetes choose appropriate CMs to achieve their treatment goals and use CMs safely. It is important to explain any risks that might occur if they do not follow management recommendations for conventional medicines and CM use. GPs can co-develop an individualised diabetes care plan, as outlined below.
- Check for interactions and side effects on Medline Plus, Natural Standards database or Natural Medicines database.
- Help the person decide their goals for using CMs and selecting relevant CMs to meet their goals (e.g. using massage, meditation and/or counselling to manage pain and distress).
- Have a correct diagnosis before using any therapy.
- Ask patients about CM use at each consultation and encourage patients to inform their GPs and CM practitioners about all the therapies they use.
- Ask patients to keep a list of all the CMs and therapies they use and to update it regularly.
- Monitor the effects on a patient’s diabetes, for example, blood glucose, lipids and HbA1c levels, as well as their response according to the reason they chose the CM (e.g. to manage pain or spiritual distress at the end of life).
- Explain that some CMs may take longer to show an effect than conventional medicines and some CMs should not be used continuously for long periods of time. Some GPs recommend ceasing the CM if there is no desired effect after two months.
- Help people find unbiased information about the CM they are interested in and provide counselling to check the veracity of information they find in chat rooms on the internet and advertising material (recommended websites include Medline Plus and Better Health Channel).
- Recommend people buy products that are approved and, if relevant, for which safety information is available.
- Inform older, very young, pregnant or breastfeeding patients and those who have kidney or liver damage or who are using a lot of other therapies that they could be at increased risk of adverse events if they use CMs, how to identify such events and what action to take if an adverse event occurs.
- Advise patients about storing and maintaining CM products appropriately and to consider safety issues if children and confused elderly people are part of the household. This also applies to storage of products in healthcare settings.
- Suggest patients seek advice about how to manage their CM (and conventional care) if they need surgery or an investigative procedure, especially if radiocontrast media are required and if any of the following occur:
– hypo/hyperglycaemia
– mental changes
– abdominal pain
– skin rashes
– nausea, vomiting, diarrhoea.
GPs could refer their patient to a reputable CM practitioner if they do not have the knowledge, competence and/or experience to feel comfortable providing advice about CMs. See Box for examples of documented benefits of CMs for people with diabetes.
{kind=link}
Summary
Many people with diabetes use CMs. GPs are in an ideal position to ask about, assess and monitor CM use. It is essential that GPs ask their patients with diabetes about CM use as a part of safe, comprehensive diabetes care. ET