Thyroid disorders in pregnancy and postpartum


Thyroid diseases
Health problems in pregnancy
Thyroid dysfunction is a common problem in pregnancy. Untreated thyroid disease in pregnancy is associated with an increased risk of adverse maternal and fetal outcomes. Thyroid function should be optimised before conception or as early as possible in pregnancy. Guidelines on the treatment of subclinical hypothyroidism in pregnancy have recently been updated to account for new research findings.
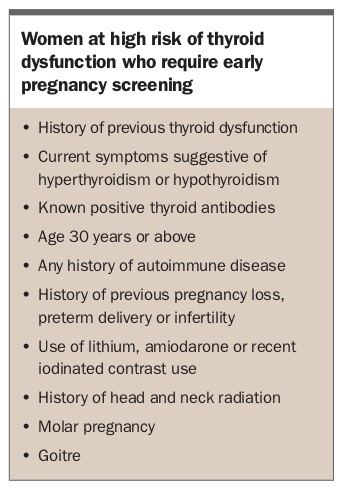
- Women at high risk of thyroid dysfunction should undergo screening with measurement of thyroid stimulating hormone (TSH) levels in early pregnancy.
- Dietary iodine intake requirements increase in pregnancy and a daily supplement containing 150 mcg of iodine is recommended to avoid iodine insufficiency.
- If the TSH level is 2.5 mIU/L or more on early pregnancy screening, levels of thyroid peroxidase antibodies should be measured to identify women who may benefit from treatment for subclinical hypothyroidism.
- Transient gestational hyperthyroidism is a common cause of mild hyperthyroidism in early pregnancy. Referral of the patient to an endocrinologist is recommended if TSH levels remain persistently undetectable and/or T3 or T4 levels are elevated and/or TSH receptor antibodies (TRAb) are positive.
- Women with active Graves’ disease or a history of Graves’ disease treated with surgery or radioactive iodine may be at risk of fetal hyperthyroidism. If TRAb level is elevated at 18 to 22 weeks’ gestation, endocrinology and maternal-fetal medicine input are required.
The fetus is dependent on maternal thyroxine (T4) in early pregnancy. The maternal thyroid gland is required to increase thyroid hormone synthesis by up to 50% to meet the increased demands of pregnancy due to placental transfer of T4, increased thyroid hormone metabolism, increased renal iodine losses and changes in levels of T4 binding proteins. These changes also affect laboratory thyroid function test assays. Thyroid stimulating hormone (TSH) is the most reliable measure of thyroid function during pregnancy. Pregnancy- and trimester-specific laboratory reference ranges should be used if available.
Whom to screen in early pregnancy for thyroid dysfunction
Current studies have not demonstrated a definite benefit from universal screening for thyroid dysfunction during pregnancy.1,2 However, women at high risk of thyroid dysfunction (Box) should have a TSH measurement before conception and as soon as pregnancy is confirmed. Free T4 and thyroid peroxidase antibody (TPOAb) testing should be performed in women with a TSH level greater than 2.5 mIU/L (see Flowchart).
{kind=link}
Iodine supplementation
Severe maternal iodine deficiency is associated with pregnancy loss, increased perinatal mortality, intellectual deficits in children and cretinism. Despite the availability of iodinated salt, mild iodine deficiency persists in Australia although this has possibly improved following iodine fortification of bread.3
During pregnancy, increased thyroid hormone production and renal losses of iodine necessitate increased iodine intake. The recommended iodine intake during pregnancy and lactation is 250 mcg daily compared with 150 mcg daily for nonpregnant adults. The NHMRC recommends a supplement containing 150 mcg iodine to be taken daily during pregnancy.4
Hypothyroidism during pregnancy
Untreated overt hypothyroidism (defined as an elevated TSH level with a low free T4 level, or a TSH level of 10 mIU/L or above regardless of the free T4 level) is seen in 0.3 to 0.5% of women of childbearing age.5 It is associated with adverse outcomes during pregnancy including increased risk of pregnancy loss, premature birth and impaired fetal neurocognitive development. All women with overt hypothyroidism should be treated with levothyroxine.2
Subclinical hypothyroidism is a milder, more common form of hypothyroidism and is defined as an elevated TSH level with a normal free T4 level. In one Australian study, 8.1% of women in early pregnancy had a TSH level between 2.5 and 5.0 mIU/L and 1.5% had a TSH level between 5 and 10 mIU/L.6 Subclinical hypothyroidism has been associated with subfertility and poor pregnancy outcomes including increased risk of miscarriage, preterm delivery, pre-eclampsia, gestational diabetes, growth restriction and premature rupture of membranes.2 The most common cause of hypothyroidism in developed countries is autoimmune thyroid disease, also known as Hashimoto’s thyroiditis. Women who are TPOAb positive have increased rates of miscarriage and preterm delivery independent of thyroid function. As a result, measurement of TPOAb levels is recommended to assist with decision making on when to treat subclinical hypothyroidism.
High-quality randomised clinical trials on levothyroxine replacement to treat subclinical hypothyroidism during pregnancy are limited. This remains an area of ongoing research. Clinical guidelines on when to treat subclinical hypothyroidism in pregnancy have changed in the past five to 10 years as more clinical trial information has become available.
The results from clinical trials of levothyroxine in pregnancy have been mixed. From an offspring neurocognitive perspective the results have been somewhat reassuring. The Controlled Antenatal Thyroid Screening (CATS)-I and CATS-II trials showed no significant difference in intelligence quotient in children aged 3 and 9.5 years of mothers with subclinical hypothyroidism randomised to levothyroxine treatment or placebo.7,8 A second randomised controlled trial similarly showed no improvement in cognitive outcomes in children of mothers treated for subclinical hypothyroidism at 5 years of age.9 A limitation of both these trials was the late commencement of levothyroxine at 13 weeks and 17 to 18 weeks of gestation, respectively.
Randomised clinical trials have shown levothyroxine replacement may reduce the rates of preterm delivery in women with subclinical hypothyroidism and positive TPOAb.10 A single trial showed that levothyroxine treatment reduced the rate of miscarriage and pre-term delivery in euthyroid TPOAb positive women.11 This result has not been replicated in subsequent studies.10,12
There is mixed evidence to suggest that treatment of subclinical hypothyroidism in women requiring assisted reproductive technology improves delivery rates.13-15
Treatment of hypothyroidism detected in early pregnancy
In women with overt hypothyroidism (TSH level >10 mIU/L), levothyroxine should be commenced and referral to an endocrinologist should be considered.
In women with a TSH level of 2.5 to 10 mIU/L in early pregnancy, the recently updated American Thyroid Association guidelines recommend evaluating for TPOAb status.2 If TPOAb positive, treatment is recommended if the TSH level is 4.0 mIU/L or above (or above trimester-specific ranges). Treatment can be considered if the TSH level is 2.5 to 4.0 mIU/L. If TPOAb negative, treatment can also be considered if the TSH level is 4.0 mIU/L or above (or above trimester-specific ranges) (see Flowchart).
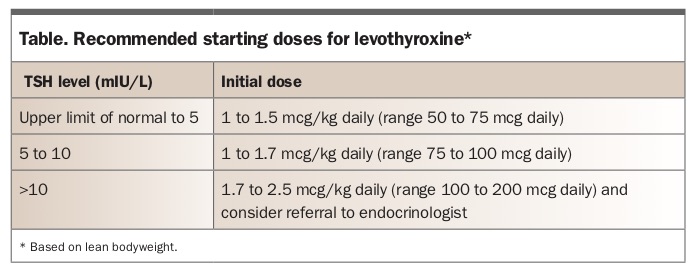
Once levothyroxine is commenced, thyroid function should be monitored four to six weekly until the TSH level is stable, then eight weekly with a final check at about 28 to 32 weeks’ gestation. Suggested starting levothyroxine doses are shown in the Table.
{kind=link}
Following delivery, the dose of levothyroxine can be halved, or ceased if on 50 mcg daily or less during pregnancy, and thyroid function checked two to three months’ postpartum.
Treatment of pre-existing hypothyroidism
Most women with pre-existing hypothyroidism will need a 20 to 30% increase in the dose of levothyroxine when pregnancy is confirmed. In patients with no thyroid tissue left (e.g. congenital hypothyroidism, post total thyroidectomy or postradioactive iodine ablation) a dose increase of 50% may be required.
Thyroid function should be monitored four to six weekly until the TSH level is stable, then eight weekly with a final check at about 28 to 32 weeks’ gestation.
Following delivery, the levothyroxine dose can be returned to the prepregnancy dose, and thyroid function should be checked two to three months’ postpartum.
Hyperthyroidism
Untreated hyperthyroidism is also associated with a range of adverse pregnancy outcomes including low birthweight, preterm birth, pre-eclampsia and stillbirth. Hyperthyroidism should be appropriately managed before conception.16
The most common cause of hyperthyroidism in women of childbearing age is Graves’ disease, which has an incidence of 30 to 80 per 100,000 person-years. Toxic nodular disease is rarer with less than two cases per 100,000 person-years.16 The incidence of Graves’ disease decreases during pregnancy due to the immunosuppressive effects of pregnancy.
Transient gestational hyperthyroidism is a common cause of mild hyperthyroidism secondary to thyroid stimulation by beta human chorionic gonadotrophin. Transient gestational hyperthyroidism is generally limited to the first half of pregnancy and is seen more often in women with hyperemesis and those with high beta human chorionic gonadotrophin levels due to molar pregnancy or multiple gestation.
If TSH levels are low during pregnancy, the TSH receptor antibody (TRAb) level should be assessed. If the TSH level is persistently undetectable and/or free T3/T4 levels are elevated and/or TRAb levels are positive then it is recommended that the patient be referred to an endocrinologist. Nuclear medicine thyroid scans are contraindicated in pregnancy.
Antithyroid medication, such as carbimazole or propylthiouracil, may be required in cases of overt hyperthyroidism. Both medications are associated with a small increase in rates of fetal malformations (2 to 4% above background rates). The birth defects associated with propylthiouracil are generally milder and more easily corrected so it is used preferentially before a planned pregnancy and during the first trimester. If antithyroid medication is required in the second or third trimesters, when the risk of malformations is lower, carbimazole is preferred due to its lower risk of hepatotoxicity. The aim of treatment with antithyroid medications is to maintain a free T4 level at the upper end (or within 10%) of the nonpregnant reference range.
Women with a history of Graves’ disease treated with surgery or radioactive iodine ablative therapy should have TRAb levels measured in early pregnancy. If positive, TRAb measurement should be repeated at 18 to 22 weeks’ gestation. As TRAb can cross the placenta and cause fetal hyperthyroidism and neonatal Graves’ disease, women with active Graves’ disease or positive TRAb at 18 to 22 weeks’ gestation should have monitoring for fetal hyperthyroidism by a maternal-fetal medicine specialist. If the TRAb level is elevated at 18 to 22 weeks’ gestation or in women with active Graves’ disease on treatment, measurement of TRAb levels at 30 to 34 weeks’ gestation can guide decisions about neonatal and postnatal monitoring.
Thyroid nodules and thyroid cancer in pregnancy
Thyroid nodules found during examination can be further assessed by ultrasound. Referral to an endocrinologist should be considered for women with nodules detected during pregnancy.
Fine-needle aspiration biopsy can be safely performed at any time during pregnancy. If differentiated thyroid cancer (papillary or follicular thyroid cancer) is detected during pregnancy, surgery can be delayed until the postpartum period as such a delay is unlikely to affect the long-term prognosis of differentiated thyroid cancer. Surgery in the second trimester may be considered for advanced differentiated thyroid cancer, medullary thyroid cancer or poorly differentiated thyroid cancer.2
Postpartum thyroid dysfunction
Postpartum thyroiditis affects 5 to 10% of women in the postpartum period and is the most common cause of postpartum thyroid dysfunction. Women with a positive TPOAb level have up to a 50% risk of developing postpartum thyroiditis and those with a past history of postpartum thyroiditis have up to a 70% risk.2,17 Postpartum thyroiditis is typically associated with transient hyperthyroidism followed by transient hypothyroidism with eventual return to euthyroidism. A quarter of women with postpartum thyroiditis have isolated hyperthyroidism and half have isolated hypothyroidism.2 Postpartum thyroiditis is a painless thyroiditis and women may be asymptomatic or have only mild symptoms of thyrotoxicosis or hypothyroidism.
In women with postpartum hyperthyroidism the main differential diagnosis is Graves’ disease, which is generally associated with a positive TRAb result and signs such as a goitre with a bruit or ophthalmopathy. In patients who develop thyrotoxicosis after six months’ postpartum, Graves’ disease is the most likely diagnosis. If there is uncertainty about the diagnosis a technetium uptake scan can be performed; however, if the mother is breastfeeding, breast milk will need to be expressed and discarded during the scan and generally for 48 hours afterwards. If antithyroid medication is required for postpartum management of Graves’ disease in breastfeeding mothers, the lowest effective dose should be used and the tablet ingested following a breastfeed. Doses of carbimazole up to 20 mg and propylthiouracil 300 mg daily have been shown to be safe in breastfeeding women with less than 1% of the parent drug being transferred into breast milk.2
Conclusion
Thyroid disorders are common during pregnancy.18,19 Early screening of at-risk women and appropriate treatment can improve pregnancy outcomes. Guidelines on the treatment of subclinical hypothyroidism in pregnancy have recently been updated to account for changes in the evidence base.2 ET