Type 2 diabetes: initiating insulin in primary care

Diabetes type 2
Diabetes medicines
The past 10 years have seen a significant increase in the therapeutic options available to people with type 2 diabetes to optimise glycaemic control. Insulin remains an important medication in the tool kit to address hyperglycaemia and reduce the risk of complications such as retinopathy, chronic kidney disease and neuropathy.
- Insulin can be safely initiated in the primary care setting. This may be facilitated by a multidisciplinary team that includes practice nurses and diabetes educators.
- Key considerations when initiating insulin include addressing patient concerns about injections and ensuring patients know the equipment that they will require, including a blood glucose meter.
- Motivational interviewing can assist in overcoming patient barriers to insulin initiation.
- GPs, practice nurses and diabetes educators can provide advice about the management of hypoglycaemia.
- All drivers need to be advised to contact the Driving Licence Authority in their state or territory to notify them of their commencement of insulin.
- It is recommended that patients register with the National Diabetes Services Scheme (NDSS) at the time of diabetes diagnosis and update their registration when an injectable therapy is commenced.
There are currently more than one million people diagnosed with type 2 diabetes in Australia,¹ most of whom have their diabetes both diagnosed and medically managed in the general practice setting. It has been estimated that 10 years after diagnosis approximately 50% of people with type 2 diabetes will require insulin injections because the beta cells in their pancreas are no longer able to produce sufficient insulin to maintain glycaemic control, even with the use of oral hypoglycaemic agents.2 For this reason, it is helpful to discuss with patients early after diagnosis their possible future requirement for insulin to maintain glucose levels in a healthy range and to explain that this is a normal part of the natural history of type 2 diabetes.
Although specialist services can be used for insulin initiation, the general practice setting may offer additional benefits to patients by providing coordination and continuity of care in their own community. In addition, patients who have chronic diseases such as type 2 diabetes value continuity for efficiency and trust that their doctor will take responsibility for their current and future care.3,4 The RACGP guidelines General Practice Management of Type 2 Diabetes include a discussion of lifestyle modifications, non-insulin medications and insulin medications and are updated regularly; the 2016–18 edition is available online (www.racgp.org.au/your-practice/guidelines/diabetes).5
Who might benefit from insulin initiation?
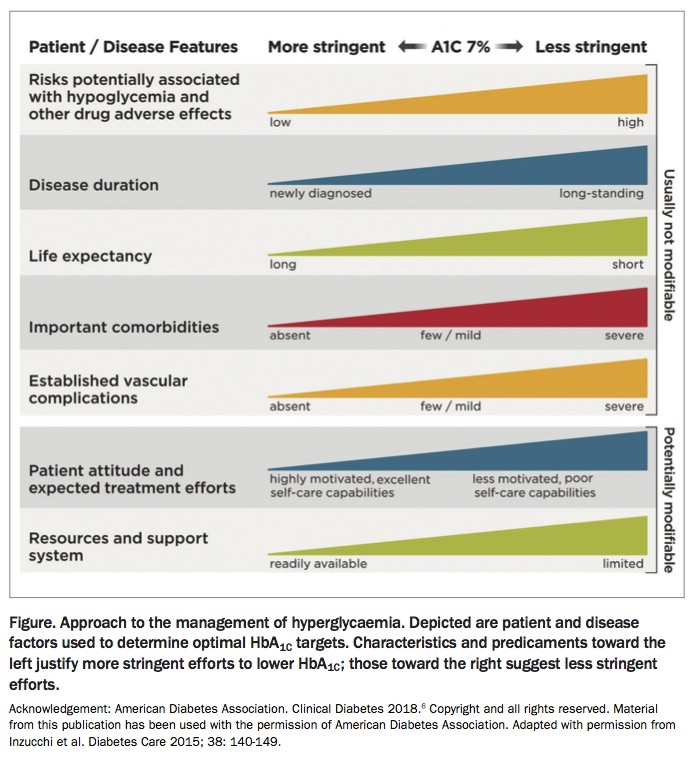
Insulin is generally used as a second-, third- or fourth-line agent in the management of glycaemia in Australia (Figure). Indications for insulin therapy in people with type 2 diabetes include:5,6
{kind=link}
- HbA1c ≥0.5% (5.5mmol/mol) above the individualised target despite maximal oral or other injectable therapy
- other glucose lowering treatments not tolerated or contraindicated
- HbA1c ≥9% (75mmol/mol), especially if a patient has symptoms of hyperglycaemia
- newly diagnosed type 2 diabetes in patients who are symptomatic and/or have HbA1c ≥10% (86mmol/mol) and/or blood glucose levels ≥16.7mmol/L.
The indications for insulin initiation need to be balanced with considerations such as disease duration, risk of hypoglycaemia, available resources and life expectancy. Together, these factors will assist in the determination of an appropriate HbA1c target.
Motivational interviewing: a tool to overcome patient barriers to insulin initiation
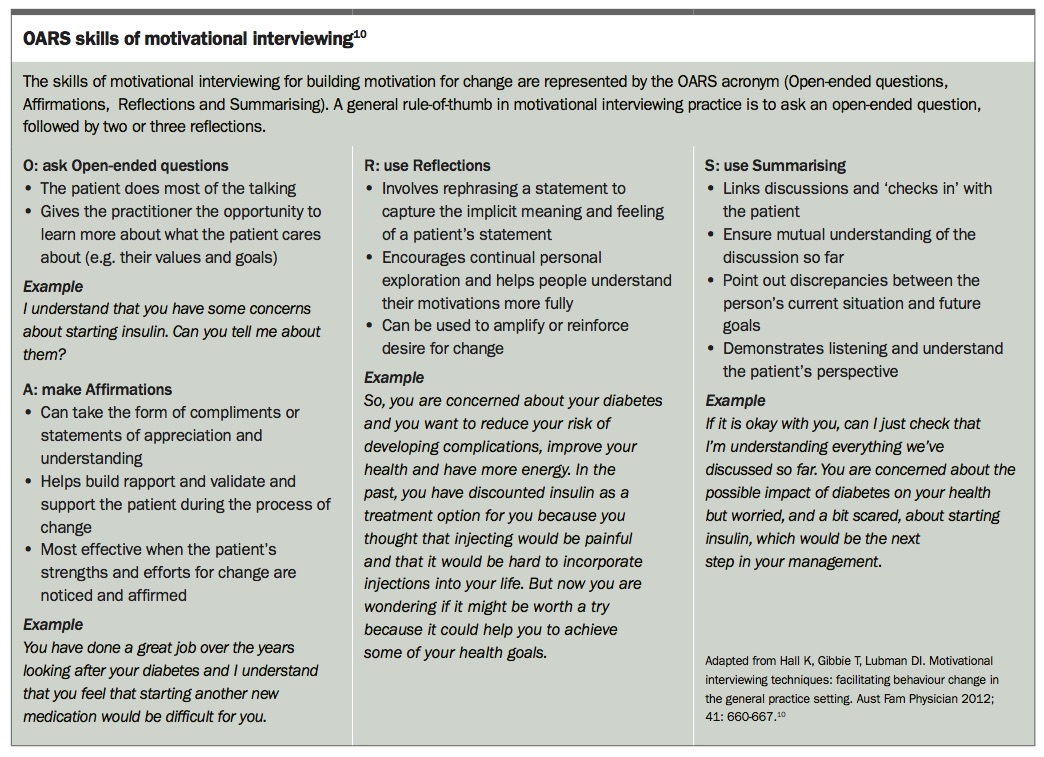
Multiple international studies have identified many patient barriers to insulin initiation. The findings are remarkably consistent, with many barriers relating to the perceived potential negative impact of insulin on life and the possible adverse effects related to the use of this medication.7-9 Use of the OARS approach to motivational interviewing, outlined in the Box, is one strategy for engaging patients about commencing insulin and addressing their concerns.10 Motivational interviewing is a counselling method that enhances motivation through addressing three components – willingness to change, ability to change (confidence) and readiness for change.10
{kind=link}
Even when the decision to commence insulin therapy has been made, some people with diabetes report feelings of guilt and failure about their need for insulin. This underpins the importance of explaining to patients early in the course of the condition that insulin therapy is likely to be required and ensuring that they do not view initiation of insulin as a ‘threat’ for not meeting glycaemic targets. A range of services are used in general practice to support patients’ emotional health; additional useful resources are available for supporting emotional health of people with type 2 diabetes through the National Diabetes Services Scheme (NDSS), which is administered by Diabetes Australia (www.ndss.com.au/online-resources-for-health-professionals).
Insulin regimens: initiation and intensification options
Once the decision to commence insulin has been made, the need for blood glucose monitoring must be discussed and the insulin regimen determined. It is important that patients agree to monitor their blood glucose levels if they are to commence insulin because these readings can assist in determining the most appropriate insulin regimen and are essential to guide titration. There are two main insulin initiation and intensification options:
- basal insulin, with intensification to a basal plus insulin regimen (the addition of a rapid-acting insulin) if required
- premixed insulin (which consists of a mixture of basal and rapid- or short-acting insulins).
The most common approach to insulin initiation is to use a basal insulin, which is injected once daily, usually in the evening. Premixed insulins may be used for patients in whom fasting and postprandial glucose levels are consistently elevated and carbohydrate intake is consistent each day; however, it is important to note that dosage adjustment can be more complex and there is an increased risk of hypoglycaemia and increased weight gain.5
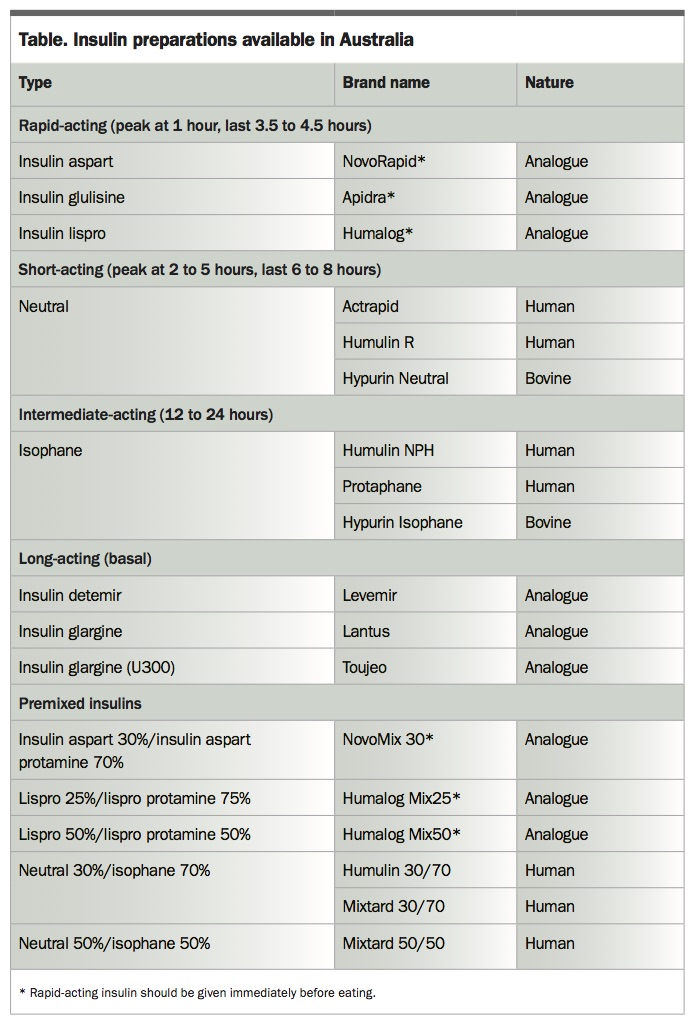
The insulins currently available in Australia and their time profiles are listed in the Table. Prefilled pen injection devices are available for all types of insulin, which can simplify patient education and injection technique. Other diabetes medications can be continued as part of both regimens, although it is common for sulfonylureas to be ceased if a rapid-acting insulin is added as part of either a basal plus or premixed insulin regimen.
{kind=link}
The general starting dose of basal insulin and premixed insulins is 10 units; however, a starting dose can also be calculated according to weight, with 0.2 units per kg per day prescribed. Suggested titration algorithms are included in the RACGP guidelines for both regimens (and available online) – the guide to starting and adjusting basal insulin is reproduced in the flowchart on page 30 and the guide to starting and adjusting premixed insulin is reproduced in the flowchart on page 31.5 The guidelines also include the basal plus titration algorithm, in which a rapid-acting insulin is added to basal insulin (and available online).5 It is recommended that insulin doses are reviewed and titrated every three days until target blood glucose levels are achieved; this can be done either face-to-face or via phone or e-mail. Patient-led titration can also be used and is safe and effective.
The current recommended target blood glucose levels are 6.0 to 8.0mmol/L for fasting glucose and preprandial glucose levels and 6.0 to 10.0 mmol/L for two hour postprandial glucose levels.11 These targets can also be individualised, with some regimens recommending tighter targets of 4 to 6mmol/L for fasting blood glucose levels, and others recommending higher targets for elderly patients and those with significant comorbidities.11
Multidisciplinary team involvement in insulin initiation
Practice nurses with appropriate training can have several roles in the initiation of insulin for patients with type 2 diabetes. These include:12
- initiating diabetes education
- assisting with the first injection
- educating the patient or carer regarding injection technique
- assisting with insulin titration, under the direction of the treating GP
- providing advice about hypoglycaemia management.
Referral of the patient to a credentialled diabetes educator (CDE) is recommended for general diabetes and self-management education as well as sick-day planning, travel advice, and assistance with blood glucose monitoring and titration of insulin. The website of the Australian Diabetes Educator Association (ADEA) has a ‘Find a CDE’ search facility for locating CDEs in a particular area, and includes information about an educator’s areas of interest (www.adea.com.au). Dietitian referral is helpful to understand the impact of carbohydrates on blood glucose levels and insulin dose.
Endocrinology review is recommended for patients with complex needs and patients who are not responding to therapy as expected. It also recommended for patients who are not achieving target HbA1c or who have required rapid escalation to insulin therapy (and so might have latent autoimmune diabetes of adulthood, for example, rather than type 2 diabetes).
Important clinical considerations in the general practice setting
Needle phobia and concerns about injection
Patient concerns about needles, pain with injection and complexity of the injection process can be overcome by having some insulin pens and needles available so the first injection can be administered under supervision in the clinic. To reduce anxiety, this is ideally offered on the day that the decision to commence insulin is made. The use of 4mm needles is recommended for injection, and patients should be aware that a new needle should be used for each injection. Principles about subcutaneous injection technique are summarised in Clinical Guiding principles for subcutaneous injection technique 2015, a useful document from the ADEA that is available online (www.adea.com.au/wp-content/uploads/ 2015/11/Injection-Technique-Final-digital-version2.pdf).13
Driving
All people commencing insulin need to be advised to contact the Driving Licence Authority (DLA) in their state or territory to notify them of their commencement of insulin. Commercial drivers are required to have an annual review with an endocrinologist or consultant physician specialising in diabetes. People with a private licence are required to have a two-yearly review with their treating doctor (which may be their GP).14 GPs are also advised to check the local requirements of the DLA in their state or territory. People with diabetes who are prescribed hypoglycaemic medications or insulin should be advised to test their blood glucose level before driving and every two hours while driving to ensure that their blood glucose level is ≥5mmol/L. Information for patients about diabetes and driving is available on the Diabetes Australia website (www.diabetesaustralia.com.au/driving).
Hypoglycaemia
Although practice nurses and CDEs can provide hypoglycaemia education, GPs commencing insulin also have a responsibility to do so. Helpful patient handouts on the management of hypoglycaemia are available on the Diabetes Australia website (www.diabetesaustralia.com.au/hypoglycaemia).
National Diabetes Services Scheme registration
GPs, CDEs and endocrinologists are encouraged to register patients with the NDSS at the time of diagnosis and to update their registration when an injectable therapy is commenced. This provides access to services such as group support programs and subsidised products such as glucose test strips and needles. Forms can be downloaded from the NDSS website (www.ndss.com.au/registration). Fact sheets and other online resources for patients and healthcare professionals are also available from the website.
Equipment
In addition to injection devices and needles, a glucose meter is essential for monitoring of blood glucose levels to inform insulin titration, identify hypoglycaemia and facilitate sick-day management. It is also important for patients to have sharps disposal units; these can be accessed through local councils or pharmacies. Ready access to food or drinks to treat hypoglycaemia is also required. GPs can consider having some injection devices and needles available at the clinic to teach injection technique.
Conclusion
Insulin initiation in general practice is feasible and safe. There are many resources available to assist GPs, and the multidisciplinary team more widely, to commence insulin in the general practice setting. Access to these resources will assist in patients having more timely intensification of their therapy, resulting in better patient outcomes. ET
COMPETING INTERESTS: Associate Professor Furler has received unrestricted educational grants for research support from Roche, Sanofi and Medtronic. Professor O’Neal and Dr Manski-Nankervis have had various financial relationships with pharmaceutical industries outside the submitted work including consultancies, grants, lectures, educational activities and travel.