Hypersensitivity reactions to monoclonal antibody treatments for immune disorders

Immune system and disorders
The use of monoclonal antibody therapies is exploding in areas such as immunology, rheumatology and gastroenterology. Although these drugs are currently prescribed only by specialists, GPs may be called on to recognise and manage adverse events following their administration.
Biological agents, encompassing monoclonal antibodies (MAbs), fusion proteins and cytokines, have become ubiquitous treatments in modern medical practice.1 Most medical specialties have at least one biological therapy in use or in the pipeline. With the increasing use of therapeutic MAbs, more patients are experiencing adverse effects, including hypersensitivity reactions. GPs must be able to recognise the adverse effects of MAbs and refer patients for review if required.
This article provides an overview of hypersensitivity reactions to MAbs, focusing on the agents commonly used in immunology, rheumatology and gastroenterology practice. MAbs used in other areas of practice, such as oncology, and other adverse effects such as infections and malignancies associated with MAb use are not addressed here.
What are monoclonal antibodies?
An MAb is an antibody produced by a single clone of cells or cell line with a monovalent affinity. The actions of MAbs depend on the target cell or receptor, but typically they downregulate cytokines, block receptors or induce cell apoptosis.
The initial therapeutic MAbs were murine (mouse-derived). Most of those used today are one of three types:
- chimeric – with murine variable regions and human constant regions (denoted by the suffix ‘ximab’)
- humanised – with murine hypervariable regions grafted onto the amino acid domains of human antibodies (denoted by ‘zumab’)
- fully human (denoted by ‘umab’).
Human MAbs are considered less immunogenic but can still elicit unwanted responses.
Types of hypersensitivity reactions to MAbs
Both immediate and delayed reactions have been described following MAb treatment. Immediate reactions occur through three main mechanisms, as follows.
- Ig (immunoglobulin) E-mediated reactions – these may occur with the first exposure to MAbs, caused by pre-formed antibodies, but onset is usually after the second or later infusions. The initial exposure allows specific IgE antibodies to form and trigger typical allergic reactions with subsequent infusions.
- IgG-mediated reactions – two mechanisms are proposed by which IgG may cause hypersensitivity reactions to MAbs.
- Cytokine-mediated reactions – binding of the MAb to its target cell results in lysis of the cell, leading to cytokine release.
Specific reactions may be caused by mixed mechanisms.
Delayed hypersensitivity is a cell-mediated response that typically presents seven to 21 days after exposure. It depends on the presentation of the MAbs by antigen-presenting cells to T cells, triggering a cytotoxic reaction. Subsequent infusions result in a more rapid onset of symptoms.
Manifestations of hypersensitivity to MAbs
Immediate hypersensitivity
Immediate hypersensitivity reactions to MAbs (mediated by either IgE or IgG) present similarly to other immediate hypersensitivity reactions, with the typical spectrum of symptoms ranging from mild cutaneous urticaria to overt anaphylaxis. These symptoms usually occur with infusions subsequent to the first.
Injection site reactions
Injection site reactions are a common adverse effect of MAb treatments that are administered by subcutaneous injection, such as most TNF inhibitors, with an incidence ranging from 1% for golimumab to 14% for certolizumab.3,4 Most of these reactions occur early in the treatment course, are mild and rarely lead to cessation of medication. Injection site reactions can be antibody-mediated or T cell-mediated. Symptoms include burning, pain, itch, swelling and redness around the injection site. These symptoms may occur immediately but usually develop within 24 to 48 hours after the injection.5
Infusion reactions
Infusion reactions can be acute or delayed and vary in presentation.
Acute infusion reactions
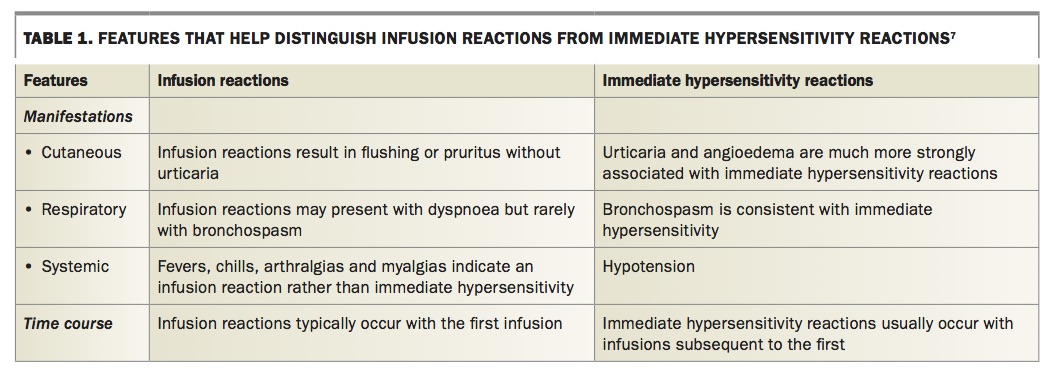
Acute infusion reactions occur within 24 hours after MAb administration, but typically between 10 minutes and four hours afterwards. They are postulated to be cytokine-mediated. They can present with a variety of symptoms, which can be cutaneous (erythema, flushing, pruritus), cardiovascular (chest pain, tachycardia, pre-syncope, syncope, hypotension), respiratory (shortness of breath), gastrointestinal (nausea, vomiting, diarrhoea, abdominal pain) and neurological (confusion, visual disturbances, numbness, weakness).6 It can be difficult to distinguish acute infusion reactions from immediate hypersensitivity reactions. Clinical features that may help determine the type of reaction are shown in Table 1.7 Identifying the type of reaction will help in deciding how to manage it.
{kind=link}
The frequency of acute infusion reactions differs between MAbs. Published reports suggest the rate is up to 40% for rituximab.5 Variation may be due to the level of humanisation of the individual MAb, as fewer reactions are seen with humanised MAbs such as tocilizumab than with chimeric or murine MAbs such as rituximab. The severity of acute infusion reactions is generally mild to moderate, with severe reactions seen less frequently. In one study, 51% of acute infusion reactions were rated as mild, 21% moderate and 17% severe.8
Delayed infusion reactions
Delayed infusion reactions occur between 24 hours and 14 days after MAb administration, but typically within five to seven days.1 Delayed infusion reactions present as a serum sickness-like illness, with arthralgias, fevers and malaise. The incidence of delayed infusion reactions is much lower than the incidence of acute infusion reactions. Delayed infusion reactions are usually self-limiting and have a good prognosis, even with repeat infusions.
Anti-drug antibodies
Although IgG antibodies can be implicated in immediate hypersensitivity reactions, they more frequently act by neutralising the active drug leading to reduced efficacy.7 Clinically this presents as loss of control over a disease that was previously well controlled. Anti-drug antibodies are particularly associated with tumour necrosis factor (TNF) inhibitors; they are detectable in 10 to 50% of patients exposed to infliximab and 25 to 30% of those exposed to adalimumab.7
Examples of reactions to specific MAbs
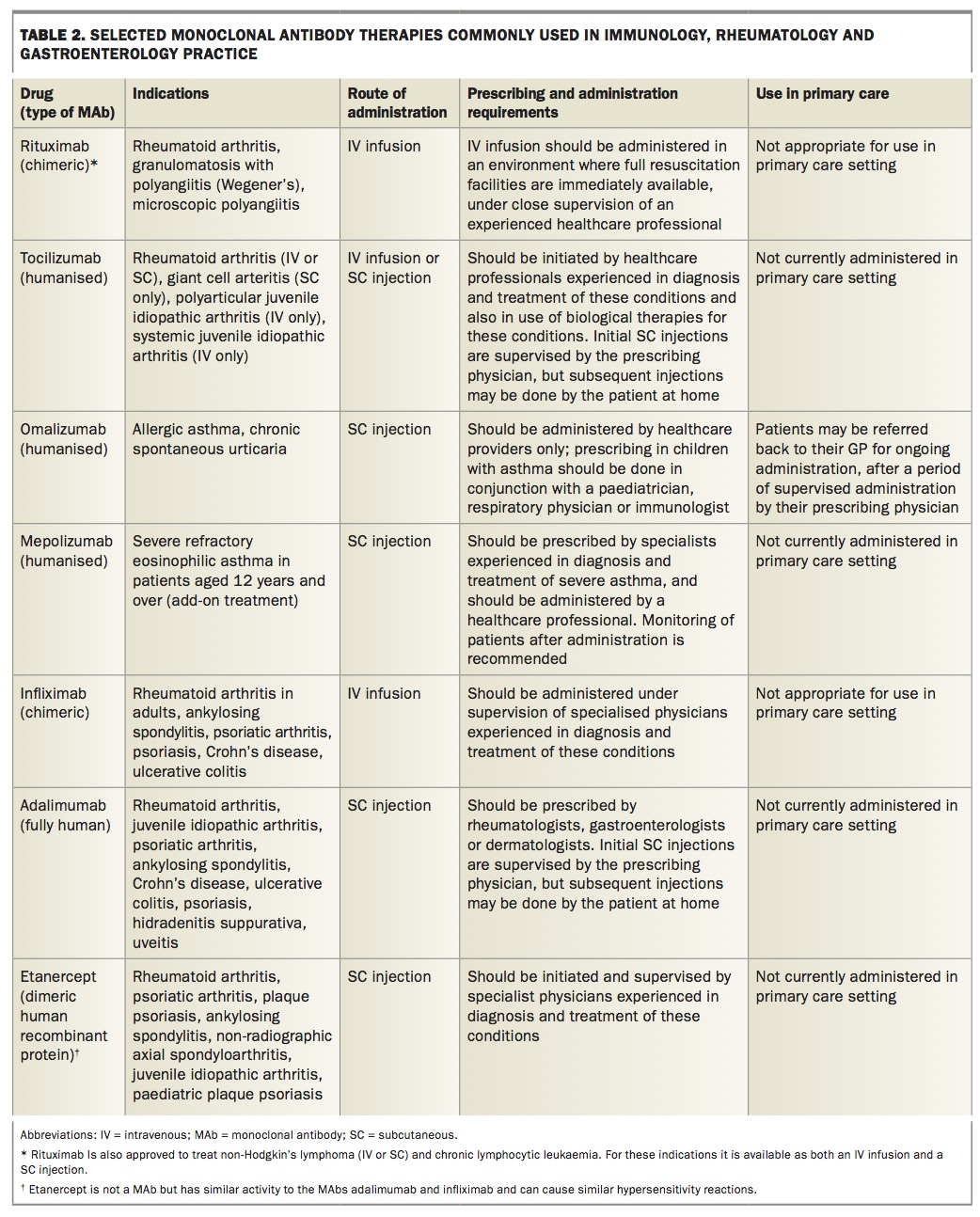
Some features of selected MAb therapies commonly used in immunology, rheumatology and gastroenterology practice are shown in Table 2.
{kind=link}
Rituximab
Rituximab is a chimeric anti-CD20 MAb used for the treatment of rheumatoid arthritis and several other inflammatory and immunological diseases. It commonly causes infusion reactions (29 to 40% of patients), and most occur with the first infusion.5 These reactions are mostly associated with cytokine release in response to the infusion. There is some evidence of anti-drug antibodies, but these would have a role in reactions following the initial infusion, and it is unclear whether they are IgG or IgE. Skin prick testing, using the MAb as the reagent, gives positive results in some patients who have IgE-mediated reactions, but these are the minority of patients who have an acute reaction. Those with negative results to skin prick tests can go on to have subsequent reactions.
Tocilizumab
Tocilizumab is a humanised MAb that targets the interleukin (IL)-6 receptor and is used to treat rheumatoid arthritis and some other inflammatory disorders. In a study of 72 patients taking tocilizumab, 20 discontinued treatment, five because of hypersensitivity and seven because of other adverse effects.9 The patients who had hypersensitivity reactions had negative results to the MAb on skin prick testing but positive results on intradermal testing. All reactions occurred with the second or later infusions, which suggests the reactions are IgE-mediated.
Omalizumab
Omalizumab is a humanised anti-IgE MAb used in the management of severe allergic asthma and severe chronic spontaneous urticaria. As omalizumab is given subcutaneously, the vast majority of reactions are injection site reactions (45%). Anaphylaxis is rare but has been reported in 0.2% of patients.10 Most anaphylactic reactions (68%) occur within the first three administrations of the drug.5 Delayed presentations of anaphylaxis have also been recorded, with 5% of cases occurring more than one day after administration.6
Use of omalizumab for chronic spontaneous urticaria is recent. Most cases of anaphylaxis have been reported in patients receiving treatment for severe uncontrolled asthma. Individuals at risk of anaphylaxis from other causes appear to have greater risk of this adverse effect. For this reason, omalizumab is not available for patients to self-inject at home. Monitoring is advised for two hours after the first injection and for one hour thereafter. In some centres, patients considered to have a higher risk are prescribed an adrenaline (epinephrine) autoinjector with appropriate training and are instructed to have it available at the time of injection and for 24 hours after the injection. Omalizumab injections should be given under the supervision of a medical practitioner.
Mepolizumab
Mepolizumab is a humanised MAb that targets IL-5, blocking binding of the IL-5 receptor on the surface of eosinophils and thereby preventing eosinophil development and activation.11 It is used in the management of severe eosinophilic asthma. It is given subcutaneously and is generally well tolerated. Approximately 8% of patients have injection site reactions. There have been no reports of anaphylaxis to mepolizumab, but 1% of patients in clinical trials had symptoms consistent with hypersensitivity (e.g. rash).11
Tumour necrosis factor-alfa inhibitors
The TNF-alfa inhibitors are the largest and best studied group of MAbs. In addition to their use in immunology and rheumatology, they are commonly used in gasteroenterology practice. The hypersensitivity profile varies between the different drugs. MAb TNF-alfa inhibitors include adalimumab, certolizumab, infliximab and golimumab. Representative reactions to TNF-alfa inhibitors are described below, but the list is not exhaustive. Etanercept is another TNF-alfa inhibitor that is not a MAb but has similar potential to produce hypersenstivity reactions. The subcutaneous TNF-alfa inhibitors are most commonly self-administered by patients after appropriate training.
Infliximab
Infliximab is a chimeric MAb, with a murine variable region bound to the Fc region of human IgG; it is given by intravenous infusion. Adverse reactions occur in 3 to 22% of patients receiving infliximab for psoriasis, and usually occur within the first two hours after the infusion.5 Anaphylaxis is a rare reaction. The reported cases usually occur after several infusions, suggesting the development of anti-drug antibodies. Levels of antichimeric antibodies can be checked, and the development of these may also be related to loss of treatment efficacy.
Adalimumab
Adalimumab is a recombinant human IgG1 MAb that is administered by subcutaneous injection. The most common reported reaction is a mild injection site reaction (20%).5 Rare cases of more severe reactions have been reported after repeat injections. Some of these patients had positive results to the MAb on skin prick and intradermal testing.
Etanercept
Etanercept is a TNF-alfa inhibitor that is a dimeric human recombinant protein rather than a MAb. Like the MAb TNF- alfa inhibitors, it is administered by subcutaneous injection and can elicit similar hypersensitivity reactions. It has been associated with the production of anti-drug antibodies in approximately 18% of patients after long-term use, and various allergic skin eruptions have also been reported.5
Management
The mainstay of management of acute reactions to MAb therapy is adequate monitoring to detect the reactions in the first instance. Infusion centres have protocols to address the appropriate administration of these medications. These protocols outline any required pre-medication, the rate of intravenous infusions and the management of adverse events. Management depends on the likely mechanism or type of reaction.
Injection site reactions
Symptomatic injection site reactions can be treated with ice or topical local anaesthetics.8 For persistent symptoms, topical corticosteroids can be of some benefit. Initial subcutaneous injections of a MAb are typically given by trained nursing staff, who then monitor patients for a specified time after the injection to assess for a reaction. After training and an uneventful supervised injection, a patient can self-administer MAb therapy at home, depending on which MAb they are receiving. At present, omalizumab must be given in a medical facility as postinjection monitoring is required.
Infusion reactions
The first infusion of a MAb is typically undertaken incrementally, with the rate of infusion increased slowly to the maximal rate, as long as it is tolerated by the patient. Most acute infusion reactions to MAb therapy such as rituximab respond well to ceasing the infusion until the symptoms resolve, then restarting at a slower rate. Infusion centres have protocols for pretreatment before infusion of a MAb that are aimed at preventing or minimising the severity of any acute reactions. Pretreatment regimens involve intravenous hydrocortisone and high-dose second-generation antihistamines, such as cetirizine 20mg.
Patients who experience a delayed infusion reaction may present to their GP. Usually, they do not require specific management.8 Most symptoms are mild and flu-like, and respond well to simple analgesia such as paracetamol. Patients with persistent or severe joint pain may require a short course of corticosteroids. If a patient’s symptoms are more severe or do not settle with simple analgesia then their condition should be discussed with the prescribing physician.
Immediate hypersensitivity reactions (subcutaneous and intravenous MAbs)
Initial management of patients with an immediate hypersensitivity reaction involves cessation of the infusion (if intravenous) and administration of antihistamines, with adrenaline if required. If an IgE-mediated reaction is suspected rather than an acute infusion reaction for a MAb administered intravenously then assessment is required before the next infusion. Skin prick testing using dilute, nonirritating preparations of the MAb may be useful in assessing the presence of anti-drug IgE antibodies.2
For patients with recurrent or severe acute infusion reactions or allergic reactions confirmed by positive skin test results and for whom the MAb treatment is vital or a last resort, there are options for acute desensitisation.12 Desensitisation is performed only under specialist supervision. Desensitisation protocols vary between practices but generally involve introducing the patient to the medication, beginning with very low doses, and increasing the rate more slowly than is usual for infusions, until the prescribed dose is completed. Desensitisation is used when the patient is expected to have repeat administrations of the MAb, as repeat exposure is required to maintain tolerance.
IgG anti-drug antibodies
Some MAbs, such as TNF alfa inhibitors, have an increased risk of causing the development of anti-drug antibodies, which may predispose patients to reactions with repeat dosing. For these patients, the prescribing specialist may consider commencing therapy with immunomodulators such as thiopurine or methotrexate to prevent the production of the antibodies. The use of immunomodulators has also been shown to reduce anti-drug antibody levels in patients with detectable antibodies who have lost clinical response to the MAb.13
Summary
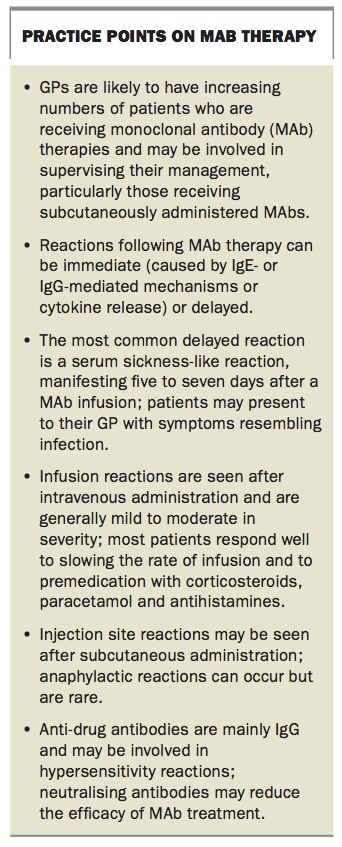
Prescription, administration and initiation of MAb therapy remains the purview of specialist physicians at present. However, given the explosion in use of these agents across a variety of areas of medicine, all clinicians require at least a basic understanding of the mechanism of action of these drugs and the presentation of adverse events. Some practice points on MAb therapy are summarised in the Box. GPs may be called on to recognise and manage adverse events following administration of a MAb. Some reactions are predictable and easily addressed (e.g. injection site reactions and infusion reactions), but patients with a suspected immediate hypersensitivity reaction or recurrent severe infusion reactions require referral back to the prescribing specialist for re-evaluation. MT
{kind=link}