Investigating primary aldosteronism

Adrenal gland disorders
Hypertension
There are clear criteria for screening and diagnosis of primary aldosteronism. Initial screening includes measurement of the aldosterone-to-renin ratio and electrolytes.
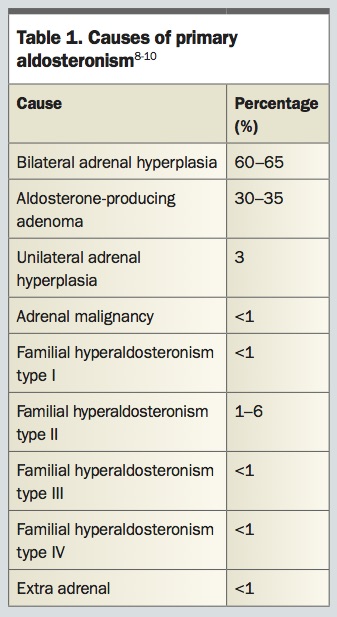
PA predominantly arises from bilateral adrenal hyperplasia (BAH) or an aldosterone-producing adenoma (APA); the latter is more classically described as Conn’s syndrome. PA may rarely result from adrenocortical carcinoma or familial syndromes (Table 1).8-10 Contrary to traditional teaching and early epidemiological studies suggesting predominant unilateral disease due to an APA, bilateral disease accounts for the majority of cases of PA, with significant implications for work-up and management. APA is amenable to surgical resection, whereas BAH is not but may be effectively managed medically.8
{kind=link}
Over the past decade, considerable knowledge has been gained in regard to the molecular basis of PA. Most notably, KCNJ5 somatic mutations have been found to be present in 40% of Caucasian patients and in 60 to 80% of Asian patients with APAs.3-11 However, despite identification of such somatic mutations, genetic studies currently have little role in the management of APAs because they do not affect treatment plans.8
The deleterious consequences of PA on the cardiovascular, cerebrovascular and renal systems extend well beyond the pure effects of hypertension.12 In a study comparing the frequency of cardiovascular events against matched patients with primary hypertension, PA was associated with increased left ventricular volume, myocardial fibrosis and an increase in cardiovascular events such as myocardial infarction, atrial fibrillation, heart failure and cerebrovascular accidents.3,12 In addition, it may increase the risk of metabolic syndrome, diabetes and bone loss.10 Patients with PA have higher rates of left ventricular hypertrophy and other adverse cardiovascular outcomes compared with patients with essential hypertension, even when matched for age, weight, and level and duration of hypertension. Such adverse effects appear reversible with specific aldosterone antagonism.13 Hence, early diagnosis, classification of subtype and treatment of PA are essential.
Case 1
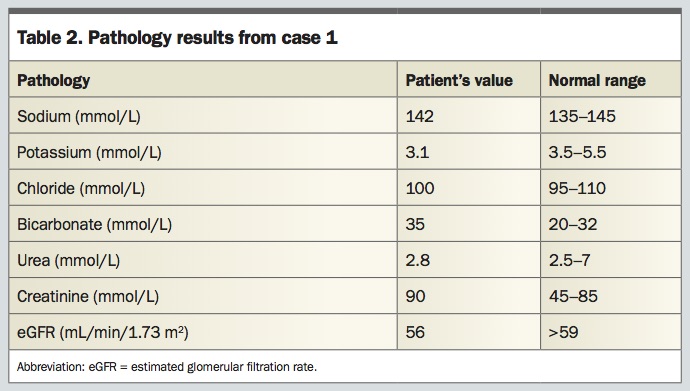
A 63-year-old man with a 20-year history of hypertension is referred to the endocrinology clinic to investigate uncontrolled blood pressure and hypokalaemia. He is currently taking valsartan/hydrochlorothiazide 160 mg/25 mg once daily, prazosin 5 mg twice daily, atenolol 50 mg once daily, in addition to clopidogrel 75 mg once daily and aspirin 100 mg once daily. On examination, his blood pressure is 167/102 mmHg and pulse rate is 65 beats per minute. Chest auscultation reveals an S4 and ophthalmoscopic examination shows arteriovenous nipping with scattered soft exudates. His initial blood test results are shown in Table 2.
{kind=link}
What is the next step?
This man has refractory hypertension despite being adherent to four antihypertensive medications. He has the classic electrolyte triad of low (or low–normal) potassium, high–normal sodium and high bicarbonate levels (metabolic alkalosis). This gives a clear indication to screen him for PA. Other less common causes of secondary hypertension also need to be excluded such as Cushing’s syndrome or phaeochromocytoma.
The best available screening test for PA is the aldosterone-to-renin ratio (ARR), which is indicated in patients with hypertension if they have one or more of the following:8
- blood pressure above 150/100 mmHg on three or more occasions
- uncontrolled blood pressure with use of three antihypertensive medications (including diuretics)
- controlled blood pressure with use of four antihypertensive medications
- adrenal incidentaloma
- a first-degree relative with PA
- spontaneous or diuretic-induced hypokalaemia
- sleep apnoea.
This case clearly meets these criteria.
What preparations should be undertaken before ARR testing?
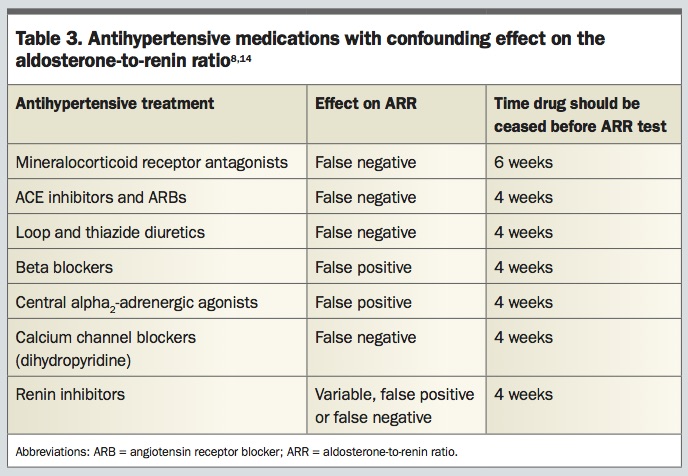
Antihypertensive medications that may affect the ARR should ideally be ceased at least four weeks before blood collection for the ARR test (Table 3).8,14 Alternative antihypertensive medications that have minimum interference on the ARR include nondihydropyridine calcium channel blockers (such as delayed-release verapamil), hydralazine, prazosin, doxazosin and terazosin.8,14 In this case, valsartan/hydrochlorothiazide and atenolol were replaced with verapamil. Stopping potentially interfering antihypertensive medications can be challenging, especially for people with refractory or severe hypertension, and should be undertaken cautiously with careful monitoring for adverse effects of hypertension. In some cases, it may be necessary to proceed to ARR testing despite the patient taking a potentially interfering medication, rather than delay testing or risk severe uncontrolled hypertension sequelae.8
{kind=link}
Hypokalaemia is a potent suppressor of aldosterone, and potassium levels of less than 4.0 mmol/L may be associated with an increased risk of a false-negative ARR ratio.14 Hypokalaemia should be corrected before testing with oral potassium supplementation, aiming for a serum potassium level of 4 mmol/L or above. Patients should avoid either sodium restriction or supplementation.8
A blood sample for the ARR test should be collected in the morning after the patient has been ambulant for two hours, and then seated for 15 minutes.14 The levels of renin is dependent on posture and its secretion is stimulated by standing. Aldosterone level is also increased with upright posture due to decreased hepatic blood flow and decreased hepatic clearance. However, collectively, the effect of posture on ARR is minimal.15 The preparations necessary before ARR testing are summarised in the Box.
{kind=link}
How to interpret the results of the ARR test
The interpretation of the ARR test can be challenging because cut-off values vary by laboratory and according to whether standard international or conventional units are used for the aldosterone and renin levels. Furthermore, renin can be measured either as plasma renin activity or direct renin concentration.
Using standard international units for aldosterone (pmol/L) and direct renin concentration (mU/L) an ARR above 70 is considered positive for PA, whereas using traditional units for aldosterone (ng/dL) and plasma renin activity (ng/ml/hr) a cut-off value of more than 20 is used. Occaionally, renin is fully suppressed meaning the ARR is elevated even when the aldosterone is low. To avoid such false-positive results, some authors suggest that an absolute plasma aldosterone concentration above 415 pmol/L should be used to consider the ARR ratio as positive.10 As mentioned above, false negatives may also occur with potassium levels less than 4.0 mmol/L or with use of certain antihypertensive medications (Table 3).
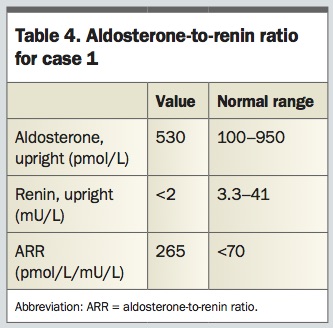
For this patient, the aldosterone, direct renin concentration and ARR are shown in Table 4. Testing of 24-hour urinary free cortisol, an overnight 1 mg dexamethasone suppression test and plasma metanephrines were normal. Accordingly, the screening test for PA is positive.
{kind=link}
How is the diagnosis of PA confirmed?
To confirm or refute the diagnosis of PA, a positive ARR screening test should be followed by a confirmatory suppression test. Options include normal saline suppression test, oral sodium loading test, captopril challenge test or fludrocortisone suppression test.8 The choice of the test depends on the patient’s clinical picture and preference, availability of expertise and cost.
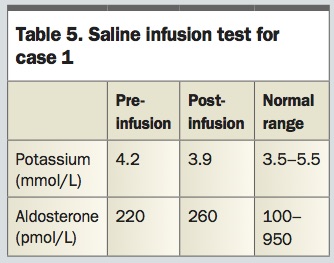
Giving its simplicity and reliability, saline suppression testing was chosen for this patient (Table 5). In this test, the plasma aldosterone concentration is measured before and after a four-hour intravenous infusion of 2 L of 0.9% sodium chloride.16 Failure to suppress the plasma aldosterone concentration below 139 pmol/L confirms a diagnosis of PA.
{kind=link}
What are the next steps?
Once a diagnosis of PA is established, the next step is to determine whether the patient has unilateral or bilateral disease. This is an essential step in the management of PA as APA is amenable to surgical resection, whereas BAH requires medical therapy.
Initially, a CT scan of the adrenals is recommended for every patient with confirmed PA.8 This helps to rule out malignancy and is a prerequisite to adrenal venous sampling (AVS); however, its role in differentiating unilateral from bilateral disease is limited due to low sensitivity and specificity.8,17 One study showed that half of AVS-confirmed cases of APA were not detected by CT scan and this figure increased to 75% for nodules less than 1 cm.10 Adrenal nodules are relatively common in the general population, especially in older age groups (10% of populations over the age of 70 years) and the presence of a nonfunctioning adrenal adenoma with superimposed BAH may occur.18 Alternatively, young patients (<35 years of age) with hypokalaemia, a high nonsuppressible serum aldosterone level and CT findings of unilateral adrenal adenoma may be offered surgery without AVS.8 Patients with an adrenal adenoma of more than 4 to 6 cm may carry a higher risk of malignancy and should have surgical excision without further PA workup.6,8,19,20 MRI has no advantage over a CT scan in detection of adrenal lesions.8
Although it is technically demanding and invasive, AVS is the most sensitive (95%) and specific (100%) test to determine lateralisation in patients with PA.21 Importantly, before proceeding with this procedure, the surgical option should be discussed with the patient and their fitness for surgery assessed. Patients who refuse or are unfit for surgery should not proceed to AVS.
AVS involves catheterisation of the left and right adrenal veins for measurement of cortisol and aldosterone concentrations.17 AVS is a technically difficult procedure and should be performed at a dedicated centre by an experienced radiologist with a view to optimising its diagnostic accuracy and minimising complication risk.5
Measuring serum cortisol levels in the cannulated adrenal vein, which is expected to be high, helps with confirmation of successful catheterisation.22 A selectivity index is calculated by dividing the cortisol concentration of the adrenal vein over a peripheral vein. A selectivity index of 3 or higher without ACTH stimulation, or more than 5 with continuous ACTH stimulation, is generally regarded as indicating successful adrenal vein catheterisation.5 For each side, an aldosterone-to-cortisol (ACR) ratio is calculated, with the ACR of the dominant side divided over the nondominant side to produce a ratio called the lateralisation index. Unilateral disease is diagnosed when the ACTH-stimulated lateralisation index is more than 4 (or more than 3 without ACTH stimulation); values below 3 support a diagnosis of BAH.8,17,23 Ratios between 3 and 4 are equivocal for bilateral or unilateral disease. In this group, addition of contralateral suppression of aldosterone as a criterion in conjunction with the finding of a solitary nodule on CT scan can confirm the diagnosis of unilateral APA with sufficient confidence to recommend surgical resection.8,24
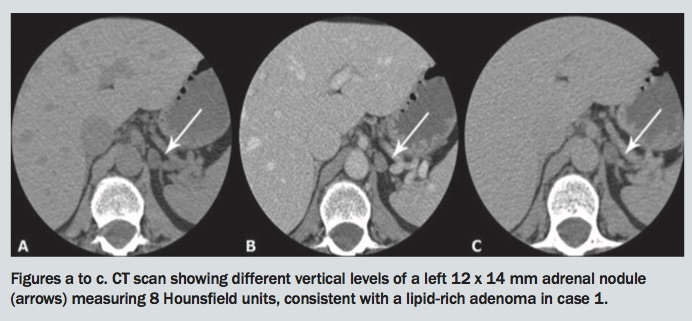
For this patient, a CT scan showed a left 12 x 14 mm adrenal nodule measuring 8 Hounsfield units, which is consistent with a lipid-rich adenoma (Figures a to c). AVS was carried out, which showed a lateralisation index of 18.5 to the left confirming a left-sided APA.
{kind=link}
How should this patient be treated?
The best treatment for this case is surgical resection of the lesion. Given its safety and short recovery time, laparoscopic unilateral adrenalectomy is the procedure of choice. Postoperatively, most patients experience resolution of hypokalaemia. Less than half attain normal blood pressure without medication although most patients do achieve significant improvements in blood pressure and/or reduction in antihypertensive therapy.25 Contributory factors to persistent hypertension include the deleterious vascular and renal effects of long-term uncontrolled hyperaldosteronism, sex-specific factors, as well as underlying essential hypertension.7,8,26
Case 2
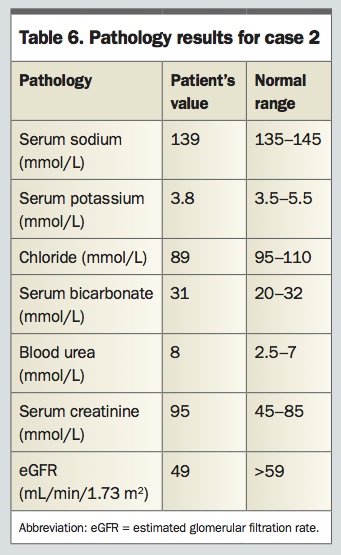
A 70-year-old man presents to the endocrinology clinic for refractory hypertension. He has had hypertension and type 2 diabetes for more than 20 years. His only complaint is nocturia three times a night. He has no known prostatic disease and his recent glycated haemoglobin level is below 7% (<53 mmol/mol). His usual antihypertensive medications are irbesartan 300 mg once daily, methyldopa 500 mg four times daily, atenolol 50 mg once daily and hydralazine 100 mg twice daily. He is adherent with this regimen. He has no family history of hypertension. On examination, his weight is 100 kg, height is 176 cm and body mass index is 32.2 kg/m2. Blood pressure seated is 160/96 mmHg. His blood test results are shown in Table 6.
{kind=link}
How should this patient’s clinical condition and biochemical tests be interpreted and what is the next step in his management?
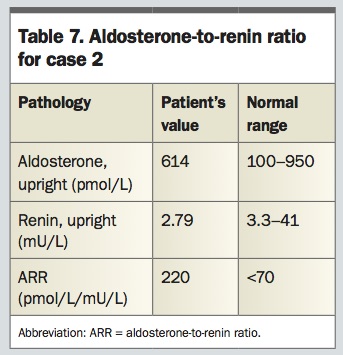
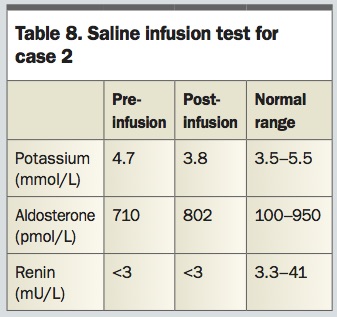
This patient has uncontrolled blood pressure despite taking four antihypertensive agents. He should therefore be screened for PA. His bicarbonate level is at the upper limit of normal, suggesting a tendency towards metabolic alkalosis, a feature of the urinary hydrogen and potassium loss characteristic of PA. Normal potassium level does not exclude the possibility of PA, as only 20% of patients with PA have persistent hypokalaemia.3 The next step is to screen him for PA using the ARR test after proper preparation. Irbesartan, atenolol and methyldopa were ceased, and the patient switched to slow-release verapamil and prazosin. The ARR was high (Table 7). Subsequently, saline infusion suppression test confirmed autonomous secretion of aldosterone (Table 8).
{kind=link}
{kind=link}
To localise the source of hyperaldosteronism, AVS was performed. The selectivity index for both adrenal veins was above 23 and lateralisation index was 1.7, confirming a diagnosis of BAH.
How should this patient be treated?
As the AVS has confirmed BAH, medical therapy with a mineralocorticoid receptor antagonist is the mainstay of treatment. Spironolactone is generally the first-line agent used with a typical starting dose of 12.5 to 25 mg/daily. The dose can be uptitrated gradually to 100 to 200 mg/daily, although generally lower doses are effective. Side effects are dose related, and include gynaecomastia, breast engorgement, menstrual irregularity and depression.8,10 Women of reproductive age must use barrier contraception due to the risk of birth defects in male fetuses (indeterminate genitalia due to androgen blockage).
Eplerenone is a second-generation selective mineralocorticoid receptor antagonist that lacks effects on androgen and progesterone receptors. Disadvantages include that it is less effective in reducing blood pressure and more expensive than spironolactone. Consequently, it is considered second line in the treatment of PA (an off-label indication). Other medications used with some scientific evidence of efficacy include amiloride and triamterene.8 Other antihypertensive agents, such as ACE inhibitors, angiotensin receptors agonists and calcium channel blockers, may be used in addition to a mineralocorticoid receptor antagonist to further control blood pressure; however, they lack specific aldosterone antagonism.8
Case 3
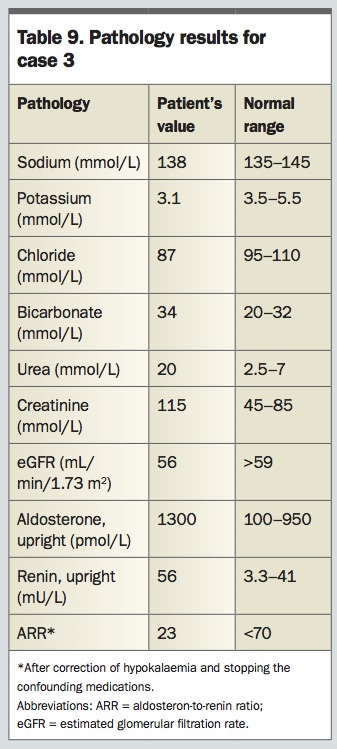
A 68-year-old woman with long-standing hypertension, type 2 diabetes and stable ischaemic heart disease complicated by heart failure presents with difficult to control blood pressure over the past several months and hypokalaemia. Her current antihypertensive medications are valsartan/ hydrochlorothiazide 160 mg/25 mg, bumetanide 1 mg, bisoprolol 2.5 mg, all once daily. Her blood test results are shown in Table 9.
{kind=link}
How should this patient be managed?
This woman has an ARR of 23, with high aldosterone and high renin levels. This represents secondary hyperaldosteronism, which is mainly caused by decreased renal blood flow producing high renin- and high aldosterone-related hypertension. Renin secretion from juxtaglomerular cells is stimulated when renal
blood flow is reduced. Renin in turn causes the cleavage of angiotensin I to angiotensin II which promotes vasoconstriction and aldosterone secretion with subsequent water and sodium retention and increased blood pressure.27 The resultant hyperaldosteronism is described as secondary in contrast to primary whereby the secretion of aldosterone is autonomous (i.e. it does not stem from renin–angiotensin pathway activation).
In this patient, secondary hyperreninaemic hyperaldosteronism can result from chronic diuresis and heart failure which cause stimulation of renin secretion via sympathetic nervous system activation.27 Renal artery stenosis is an important consideration that should be excluded, although the renin levels seen are typically higher than in this woman. Her hypokalaemic alkalosis is a diuretic effect.
The next step in this patient’s investigation would be to assess her renal arteries with duplex ultrasound or CT angiography. As outlined above, such secondary hyperaldosteronism lacks specific responsiveness to mineralocorticoid receptor antagonist therapy. She should be managed with standard therapy for hyper-tension, ischaemic heart disease and heart failure.
Summary
Primary aldosteronism is a relatively silent but deadly disorder occurring in up to 10% of patients with hypertension. Clear criteria for screening and diagnosis exist. ARR is the standard screening test for PA. Correct diagnosis, classification and management can restore normal blood pressure and greatly ameliorate cardiovascular risk. As such it is essential that GPs remain vigilant and consider this potential diagnosis in patients with hypertension, hypokalaemia or adrenal nodular disease. Initial screening should include measurement of electrolytes and ARR, and if these are abnormal, referral of the patient to a specialist for further assessment is appropriate. ET