Infected foot wound in a man with diabetes

Diabetes type 2
A 57-year-old man presents with a diabetic foot ulcer. The causes of this condition, along with appropriate management and referral options, are reviewed.
He attends your clinic with a wound on his left foot. Several weeks ago, he accidentally kicked a stool with his left foot, without pain. He initially noticed an area of redness at the impact site, but the wound later grew in size, became warm and developed into a blister. He does not feel pain in his feet and often feels like he is walking on thick carpet.
His medical history includes type 2 diabetes (diagnosed 14 years ago), hypertension, dyslipidaemia, coronary artery disease and erectile dysfunction. His regular medications include aspirin 100 mg orally in the morning, metoprolol 12.5 mg orally twice daily, extended-release metformin 1 g orally at night, perindopril 4 mg orally in the morning, rosuvastatin 10 mg orally at night, insulin aspart 4 units subcutaneously three times daily with meals, and insulin glargine 12 units subcutaneously at night. He has not been monitoring his blood glucose level and says he is time-poor and lacks motivation to exercise or attend to diet and lifestyle factors. He is an ex-smoker and drinks alcohol occasionally.
What is your initial impression?
Answer: James presents with a nonspecific injury to his left foot. Red flags include his prolonged history of type 2 diabetes and the lack of pain from the injury. His recent lack of active engagement with his GP, which has led to deterioration in his health and glycaemic control, is concerning. He was 43 years old when diagnosed with diabetes and this chronic history places him at significant risk of diabetes-related complications, including cardiovascular disease, erectile dysfunction and peripheral vascular disease. He experienced an acute myocardial infarction several years ago.
How would you direct your examination?
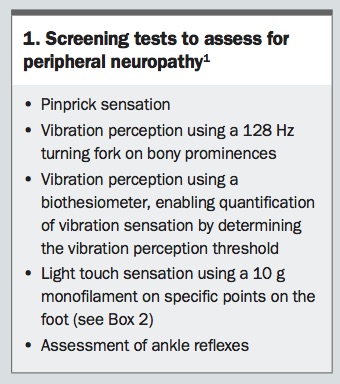
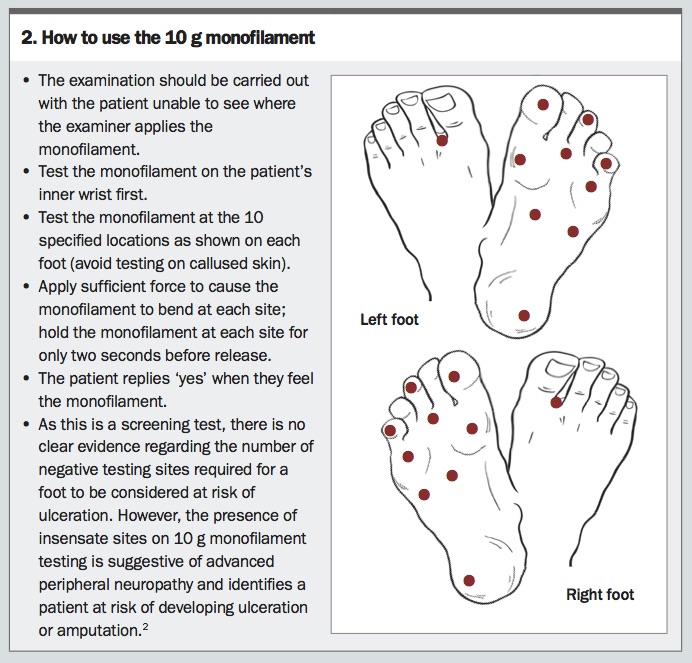
Answer: A thorough physical examination is necessary, including a screening test for peripheral neuropathy (Box 1 and Box 2).1,2
{kind=link}
{kind=link}
On examination, James appears comfortable. He is obese (body mass index, 38.9 kg/m2), with a blood pressure of 130/80 mmHg, heart rate of 80 beats/min and a body temperature of 36.5°C. A random finger-prick test gives a blood glucose level of 18 mmol/L, and ketones are undetectable.
Examination of his left lower limb reveals an ulcerated wound on the plantar aspect of the third metatarsal head (Figure 1). Dorsalis pedis and posterior tibialis pulses are faintly palpable. Pinprick testing shows that peripheral sensation is symmetrically reduced to the mid shin. Using a 128 Hz tuning fork, you find he has diminished vibration perception at the third metatarsal head.3 His ankle reflexes are diminished bilaterally.
{kind=link}
What are the immediate concerns and red flags?
Answer: A reduction in peripheral pulses is concerning and indicates the presence of peripheral vascular disease. This condition influences treatment, including the type of wound dressing and debridement, and affects the rate of tissue healing.4 Excluding critical limb ischaemia is essential by assessing for pain, pallor, pulselessness, paraesthesia and cold temperature of the limb. In the context of an open wound, an assessment of the patient’s haemodynamic stability and clinical features of septicaemia must be made. This will determine the urgency of referral for hospital-based care and intravenous antibiotics.
Despite developing a foot blister, James had continued to work, wearing gumboots daily. The continuous walking and standing in his workplace exacerbated the ulcer formation through the lack of mechanical offloading and high repetition of steps. With no preventive foot care or callus removal, the fluid from the blister contributed to the maceration of a haemorrhagic callus and subsequent ulceration.
There is a small amount of slough on the wound, which limits your ability to assess the ulcer in detail. There appears to be tendon involvement. Otherwise, there are no functional abnormalities in the toes or ankle movement. You clean the wound with saline and send a bacterial swab of the wound for culture.5
You dress the wound with cadexomer iodine, a topical ointment that removes slough and absorbs the exudate, pus and debris and forms a gel over the wound. It also has antimicrobial activity; as the ointment swells, iodine is released, leading to bactericidal activity. A foam dressing is subsequently used as a secondary dressing.
What investigations would you perform?
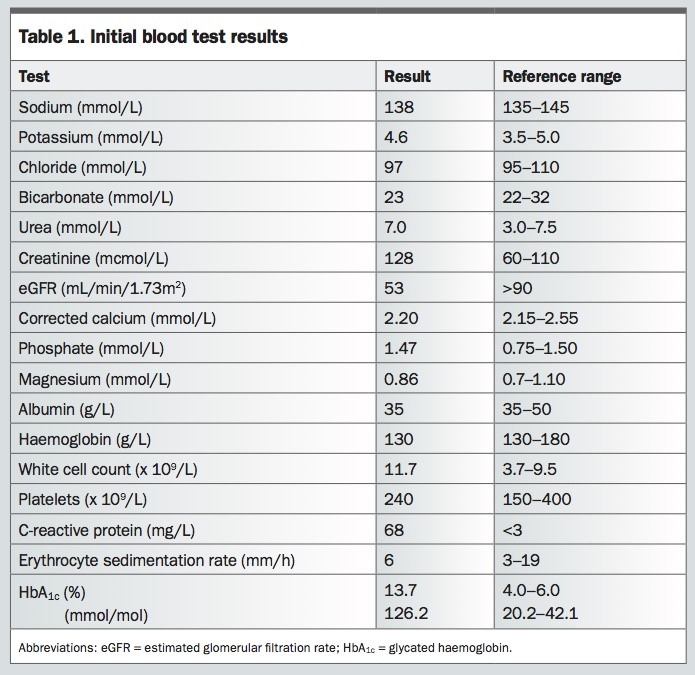
Answer: Blood tests, including full blood count, white cell count, renal function and inflammatory markers (C-reactive protein and erythrocyte sedimentation rate), should be performed. Assessing glycated haemoglobin (HbA1c) level is appropriate, as optimisation of glycaemic control is part of the treatment for foot ulcers. A bacterial swab of the wound will identify microorganisms and allow targeted antibiotic therapy.
An x-ray of the foot is essential in assessing whether underlying structures such as bone have been affected. Diabetic foot ulcers with underlying osteomyelitis may show changes on x-ray such as regional osteopenia, periosteal thickening, focal or cortical bone loss, endosteal scalloping, loss of trabecular bone architecture and, in severe chronic states, new bone apposition. If there are concerns about osteomyelitis, further imaging can be carried out. CT imaging is superior to x-ray and MRI in demonstrating the bone architecture and the development of any sequestrum or involucrum in chronic osteomyelitis,6 whereas MRI scanning is more sensitive for soft tissue and joint changes in acute osteomyelitis.
The blood test results show that James has an increased white cell count, with an elevated C-reactive protein level, suggesting infection (Table 1). His erythrocyte sedimentation rate is within the reference range. Otherwise, his results demonstrate stage 3A (moderate) chronic kidney disease. His HbA1c level is consistent with poor glycaemic control. The bacterial swab demonstrates a heavy growth of methicillin-resistant Staphylococcus aureus that is resistant to penicillin and flucloxacillin but susceptible to clindamycin. James begins taking clindamycin to treat the infection.
{kind=link}
Due to James’ history of trauma, it could be appropriate to screen for neuropathic fractures and Charcot arthropathy, in addition to osteomyelitis.
Who can you refer James to?
Answer: A foot ulcer is an acute complication of diabetes that is often underrecognised. Urgent referral of the patient to a high-risk foot clinic for wound assessment, debridement and offloading is a priority. Most of these clinics have established referral pathways to vascular surgeons, infectious disease physicians and endocrinologists. If the wound has a purulent discharge or an associated abscess, or if the patient has clinical features of septicaemia or critical limb ischaemia, referral to the emergency department would be necessary.
How do diabetic foot ulcers develop?
Answer: Patients with diabetes are at risk of several types of diabetic foot complications. Diabetic foot ulcers can be caused by a range of neuropathic, ischaemic or neuro-ischaemic processes. Diabetic neuropathy can be further subdivided into sensory, motor and autonomic loss.7
Sensory neuropathy arises from initial damage to the unmyelinated small peripheral type C fibres from chronic effects of hyperglycaemia. The loss of sensory function causes loss of protective sensation in the feet. Loss of motor nerve function leads to intrinsic muscle atrophy, which typically causes clawing of the toes and increased prominence of the metatarsal heads. Autonomic neuropathy causes reduced sweating in the foot, which leads to dry skin and may increase the risk of blister formation.
Repetitive stress and elevated plantar pressure lead to callus formation and subcutaneous haemorrhage. Peripheral vascular disease causes ischaemia, delay in wound healing and the development of a foot ulcer.
What are the underlying management principles for diabetic foot ulcers?
Answer: Five principles underpin the management of diabetic foot ulcers. These are management of the local wound, mechanical offloading, optimisation of glycaemic control, management of infection with antibiotic therapy and revascularisation of any limb affected by peripheral vascular disease.
Local wound management includes debridement of any slough or necrotic tissue in a well-perfused or healable wound. Necrotic ischaemic wounds need to be conservatively managed until reviewed by a vascular surgeon. Diabetic ulcers improve by 2.5-fold with wound debridement.8 Usually a podiatrist will carry out sharp debridement with scalpels or other debridement methods such as enzymatic, autolytic or larval therapy (Table 2, online only).8
Mechanical offloading aims to reduce or negate the pressure placed on a healing wound. The gold standard of offloading a plantar neuropathic wound is a nonremovable total contact cast. If a nonremovable total contact cast is contraindicated or unavailable, a removable total contact cast or prefabricated walker is indicated.9 These mechanical offloading measures are used in conjunction with encouraging the patient not to mobilise or bear weight on the affected limb.
Hyperglycaemia impairs immune cell and chemokine response to infection and delays wound healing by inhibiting angiogenesis and collagen formation and reducing peripheral blood flow by stasis.10 Optimisation of glycaemic control therefore assists in wound healing.
Treatment with targeted antibiotic therapy and revascularisation of an ischaemic limb support ongoing healing of a diabetic ulcer.
Are there other important but less urgent investigations you can consider?
Answer: Ensuring adequate vascular supply to the limb aids in healing a diabetic foot ulcer. In a patient with a foot ulcer and underlying diabetes, vascular supply can be assessed by an ankle–brachial pressure index, ankle and pedal Doppler arterial waveforms and either toe pressures (photoplethysmography) or transcutaneous oxygen pressure.9 A vascular surgeon may refer the patient for a CT angiogram should there be any further concerns.
James is referred to a podiatrist for review at the local high-risk foot clinic, where he is found to have a grade 2B (University of Texas classification) ulcer on the third metatarsal head of his left foot (Table 3, online only).11,12 A probe test, in which a sterile probe was inserted into the wound bed, did not hit bone, which made osteomyelitis less likely.
A general diabetes foot examination was also carried out, and the podiatrist noticed some subtle changes in the architecture of James’ right foot when compared with his injured left foot. He appeared to have some collapse of the mid tarsal arch and valgus deviation of his distal right foot. There were no obvious superficial wounds seen on James’ right foot but, because of the deformities, a baseline x-ray of the right foot was performed. The temperature difference between corresponding areas of the left and right feet was less than 2°C.
The x-ray of the right foot showed some sclerotic changes in the mid foot and pes planus deviation (Figures 2a and b). These changes suggested James had some degree of Charcot arthropathy. Usually in Charcot arthropathy, a temperature difference of more than 2°C between corresponding areas of the feet suggests active inflammation in the affected foot. However, the temperature of James’ left foot may have been elevated because of local infection and inflammation from the ulcer. Hence, James was referred for an MRI of both feet to exclude active Charcot arthropathy. His MRI showed chronic structural changes of Charcot arthropathy in his right foot. There were no changes suggesting active inflammation, microfractures or tissue swelling.
{kind=link}
What other foot complications are a risk for this patient?
Answer: In a patient with diabetes who presents with a deformed foot and pes valgus with or without pain, there is always a concern about Charcot arthropathy. Charcot arthropathy is a complex complication of
diabetic foot disease, characterised by sensory, motor and autonomic neuropathy.13 It should be suspected in patients with a history of diabetes, peripheral neuropathy and a warm to hot swollen foot or joint. This acute presentation is often misdiagnosed as a foot sprain, infection or gout. In Charcot arthropathy, longstanding peripheral neuropathy causes intrinsic muscle wasting and decreased sensation. As the biomechanics of the diabetic foot change, abnormal pressure distribution and repetitive injury cause microfractures, joint dislocation and inflammation, with progressive deformity.
Are there any other advanced treatments available?
Answer: Other advanced treatments for diabetic foot ulcers are not routinely accessible but are described in the literature. Hyperbaric oxygen therapy administers 100% oxygen intermittently to increase oxygenation to assist in wound healing. Electrical stimulation, used as an adjunctive therapy for diabetic foot ulcers, has shown some evidence of increasing the proportion of healed ulcers after 12 weeks of therapy.14 Negative pressure wound therapy has also been used successfully in diabetic foot ulcers.15 Other new therapeutic options include bioengineered skin and the use of growth factors to increase healing rates.16 Surgical techniques, such as Achilles tendon lengthening and gastrocnemius recession, have also been shown to increase ankle dorsiflexion and subsequently reduce forefoot pressure when mobilising.17 When these techniques were used in conjunction with traditional offloading to treat diabetic foot ulcers, the rates of ulcer recurrence were lower.17
James’ glycaemic control needs to be optimised to aid in healing his diabetic foot ulcer. At the initial review, James’ diabetes was managed with extended-release metformin 1 g orally at night, insulin aspart 4 units subcutaneously three times daily with meals, and insulin glargine 12 units subcutaneously at night. His HbA1c level was elevated, at 13.7% (126.2 mmol/mol), and his baseline weight was 106 kg, with a body mass index of 38.9 kg/m2. His estimated glomerular filtration rate (eGFR) was 53 mL/min/1.73 m2.
How could you optimise James’ glycaemic control?
Answer: Lifestyle advice regarding food choices and physical activity, in conjunction with pharmacotherapy, is the cornerstone of management. Depression, lack of motivation and disengagement with the healthcare profession pose common barriers to improvement in glycaemic control. Another challenge is the need for mechanical offloading, which reduces physical activity. A multidisciplinary team, including a dietitian, psychologist, diabetes educator and an endocrinologist, can provide the support needed to improve a patient’s glycaemic control.
James is already receiving the maximum recommended dose of metformin, considering his renal function. The total daily dose of metformin is adjusted according to renal function because of the concern of lactic acidosis with reduced renal clearance, especially in older patients. In general, renally adjusted metformin doses according to eGFR are 2 g daily for an eGFR greater than 60 mL/min/1.73 m2 and 1 g daily for an eGFR between 45 and 60 mL/min/1.73 m2. Metformin 500 mg daily may be considered, with caution, in patients with an eGFR of 30 to 45 mL/min/1.73 m2.
Alternative blood glucose-lowering agents that improve glycaemic control and result in weight loss, such as injectable glucagon-like peptide-1 receptor agonists or oral sodium glucose co-transporter 2 (SGLT-2) inhibitors, may be considered. One SGLT-2 inhibitor, canagliflozin, has been associated with a higher risk of amputation in patients with diabetes,18 but two others, empagliflozin and dapagliflozin, have not been associated with a similar risk. Other agents, such as sulfonylureas, are considerably cheaper but may increase weight. Dipeptidyl peptidase-4 inhibitors, such as sitagliptin, may be considered.
From the high-risk foot clinic, James is referred to a dietitian to optimise his diet and reduce his consumption of unhealthy, high-calorie foods. He is educated and provided with a meal plan that gives him options for a balanced and healthy diet. He is also referred to an exercise physiologist to establish an exercise plan, which enables James to exercise and maintain muscular strength and tone without causing elevated plantar pressure on his feet. His endocrinologist advises changes to his insulin doses, maintenance of metformin therapy and regular measurement of blood glucose levels, aiming to gradually improve his glycaemic control with regular follow up.
What further education should be provided for James?
Answer: As patients with diabetic foot ulcers experience significantly reduced quality of life and increased morbidity and mortality, education to prevent further complications or additional foot wounds is essential.19 This includes routine podiatry review and regular self-examinations of the feet. The cornerstone of managing diabetic foot disease is compliance to preventive strategies. The International Working Group on the Diabetic Foot has established guidelines for the recommended frequency of preventive screening, which are as follows:
- annually for patients without peripheral neuropathy
- every six months for patients with peripheral neuropathy
- every three to six months for patients with peripheral neuropathy, peripheral artery disease and/or foot deformity
- every one to three months for patients with peripheral neuropathy and a history of foot ulcer or lower-extremity amputation.20
Education regarding a balanced and nutritious diet is also essential, including adequate intake of vitamin C, which is needed for collagen formation and wound healing.21 Managing other risk factors associated with peripheral vascular disease assists in wound healing; specifically, smoking cessation and achieving target lipid profiles (total cholesterol level less than 4.0 mmol/L, HDL cholesterol level greater than 1.0 mmol/L, LDL cholesterol level less than 2.0 mmol/L and triglyceride level less than 2.0 mmol/L).
James’ diabetic foot ulcer was managed with a nonremovable contact cast for offloading. He continued taking clindamycin for two weeks until his wound no longer showed signs of infection. It was another two months before his wound was completely healed. The Charcot arthropathy in his right foot was closely monitored and did not show any further active inflammation. James received custom-made insoles to reduce the higher plantar pressure on the healed sites. He also received customised footwear, especially for his right foot because of the Charcot arthropathy. His podiatrist provided education and advice regarding the appropriate footwear for work, home and other daily-wear environments.
James was at risk of depression because of the biopsychosocial impact of his diabetic foot ulcer. He scored 19 out of 50 on the Kessler Psychological Distress Scale, a screening tool for depression. He was referred to a psychologist and maintained a strong therapeutic relationship with his GP. With the support around him, he continued to see his podiatrist regularly for ongoing preventive foot care and continued to work closely with his endocrinologist to optimise his glycaemic control. His most recent HbA1c level was significantly improved, at 7.8% (61.7mmol/mol). ET