Diabetic ketoacidosis

Diabetes type 1
Diabetes complications
Diabetic ketoacidosis (DKA) is a serious complication among people with diabetes that requires prompt recognition and treatment. This article describes precipitating causes and the presentation and diagnosis of DKA in adults. It provides an overview of acute management and strategies for preventing this emergency.
- Diabetic ketoacidosis (DKA) is a common complication of type 1 diabetes, and sometimes also type 2 diabetes, with associated high morbidity and mortality.
- A diagnosis of DKA classically comprises hyperglycaemia, hyperketonaemia and metabolic acidosis.
- DKA can be present in patients with only mildly elevated or normal blood glucose levels. This condition is called euglycaemic ketoacidosis and may occur with sodium-glucose cotransporter-2 inhibitors, in pregnancy or in states of impaired gluconeogenesis such as liver failure or alcohol abuse.
- Apart from measuring blood glucose levels, ketone testing should be performed and this is best done with point-of-care ketone measuring devices.
- Management objectives of DKA include fluid resuscitation and correction of hyperglycaemia, ketogenesis and acid-base imbalances. Established protocols should be used in treating DKA.
- Causes should be identified and treated, and preventive measures with sick day management plans and involvement of a multidisciplinary team should be implemented.
Diabetic ketoacidosis (DKA) is a common, acute metabolic complication of diabetes associated with significant morbidity and mortality if not promptly recognised and treated.1 The epidemiology of DKA is variable and mortality rates are subject to regional differences.2 Although DKA is classically associated with type 1 diabetes, it is now recognised that patients with type 2 diabetes may present with DKA.3 Importantly, with the introduction of sodium-glucose cotransporter-2 (SGLT-2) inhibitors, euglycaemic DKA is now a recognised entity that requires clinicians to have a low threshold of suspicion for DKA despite normal blood glucose levels.4 Position statements from the US and UK regarding the treatment of DKA are available;1,5,6 however, there are no Australia-wide guidelines.
This article describes the definition, clinical presentation, precipitating causes, diagnosis and acute management of DKA. It also outlines strategies for prevention of this common endocrine emergency. This article does not focus on hyperosmolar hyperglycaemic state, which is a complication of type 2 diabetes with a high blood glucose level (greater than 30 mmol/L) and high osmolality (greater than 320 mosm/kg) but without significant ketoacidosis. Hyperosmolar hyperglycaemic state is managed differently to DKA.
Definition of DKA
DKA comprises a triad of hyperglycaemia, increased ketones and metabolic acidosis (Figure 1).7 The 2009 American Diabetes Association diagnostic criteria for DKA are:
{kind=link}
- A plasma glucose concentration greater than 13.9 mmol/L
- The presence of ketones in urine or serum
- Metabolic acidosis, defined as arterial pH less than 7.30
- A serum bicarbonate concentration of 18.0 mmol/L or lower
- An anion gap greater than 10.1
The diagnostic criteria for DKA in the 2013 UK guidelines are:
- Ketonaemia of 3 mmol/L or more or significant ketonuria (greater than 2+ on a standard urine stick)
- Blood glucose greater than 11 mmol/L or a previous diagnosis of diabetes
- A bicarbonate concentration less than 15 mmol/L and/or a venous pH less than 7.30.6
Presentation
Patients with DKA usually present within hours to days of developing metabolic decompensation. Symptoms may include polydipsia, polyuria and weight loss. This is often accompanied by lethargy, nausea and vomiting. Physical examination may reveal dehydration, tachycardia, hypotension and sometimes a characteristic hyperventilation pattern with deep, slow breaths (Kussmaul breathing). Patients with severe dehydration may demonstrate neurological deficits.1 An associated feature is abdominal pain, which may be severe (and may be mistaken for acute pain from intra-abdominal pathology requiring surgical intervention) but usually resolves with treatment and resolution of ketosis.8
Precipitating causes
Multiple epidemiological studies have been performed to investigate the most common precipitating causes of DKA.9 The most common cause of DKA presentations to a tertiary Australian hospital was missed insulin (40%), followed by infection (29%), new diagnosis of diabetes (6%) and other causes (3%).10 A more recent study showed similar findings of precipitating factors: insulin omission (42%), infection (29%), psychosocial stressors including illicit substance use (6%), recent changes in insulin regimen (3%), epileptic seizures (1%), radiotherapy treatment (1%) and corticosteroid use (1%). No clear cause was found in 17% of patients in this study, and 23% had been diagnosed recently with diabetes.11
Initial diagnostic measures
When patients with a background of diabetes present feeling unwell the suspicion of DKA should be high. In particular, it is important that patients with type 1 diabetes who develop vomiting receive prompt medical attention. A targeted history should be taken regarding missed insulin and problems with appropriate storage or administration of insulin. An increasing number of patients with type 1 diabetes receive insulin via continuous subcutaneous insulin infusion (CSII) systems. Adverse effects, including pump failure and infusion set or infusion site-related adverse effects such as occlusion, are common and can lead to DKA. Patients on CSII who present feeling unwell must have their pump and insertion site checked by a healthcare professional familiar with CSII. If the suspicion for DKA is high the patient’s pump should not be relied on for insulin delivery until it has been checked for errors and lines have been changed.12
Depending on the patient’s age and comorbidities, other potential precipitating events need to be investigated, including infection, trauma, acute conditions requiring surgery and cardiovascular events. In addition, a careful medication history should be taken. Drugs such as corticosteroids, atypical antipsychotics or sympathomimetics and increased alcohol consumption or illicit drug use may precipitate DKA and should be considered. A new diagnosis of diabetes should be considered in patients presenting with symptoms such as polydipsia, polyuria and weight loss for the first time.9
If there is suspicion of DKA, blood glucose and ketone levels should be measured. We recommend point-of-care fingerprick ketone testing for beta-hydroxybutyrate (beta-HB), the major ketone body in blood. This provides an accurate measure of severity and recovery. Beta-HB is converted to acetoacetic acid, which is excreted via the kidneys and is the major urinary ketone. The time-lag between conversion and excretion in the urine means urinary ketone testing tends to underestimate the severity of DKA at presentation and may also give a false indication of a slower time to resolution of ketoacidosis. Further, the dehydration associated with DKA may result in oliguria with a delay in diagnosis if relying on urine ketone measurements.13
Importantly, despite most patients with DKA presenting with elevated plasma glucose levels, some patients will exhibit only mild elevation of their plasma glucose.9 This euglycaemic DKA is becoming more frequent with the widespread use of SGLT-2 inhibitors. Therefore, all patients with diabetes who experience nausea, vomiting or malaise or develop metabolic abnormalities in the setting of SGLT-2 inhibitor therapy should be evaluated for DKA.14 Euglycaemic DKA is also observed during pregnancy and in patients with impaired gluconeogenesis due to alcohol abuse or liver failure.15,16
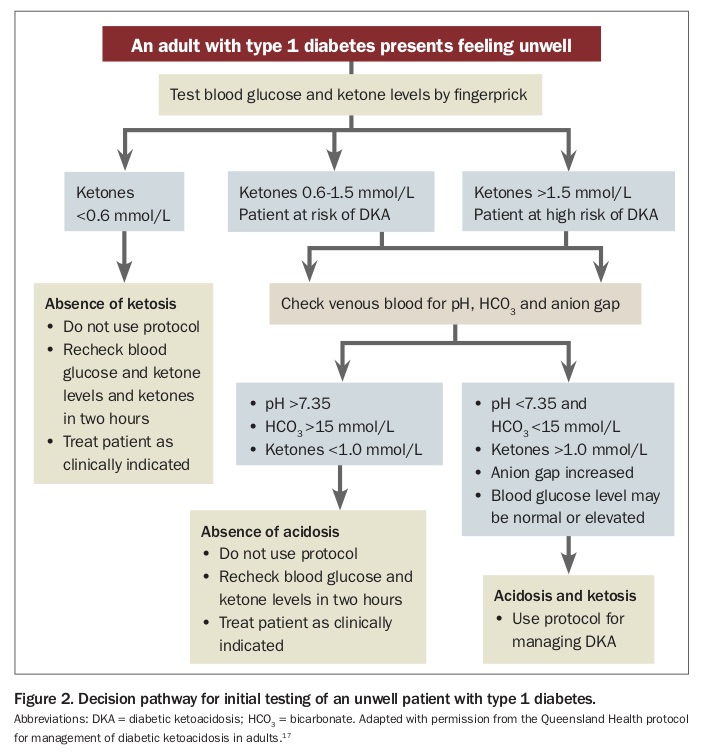
GPs usually do not have access to rapid laboratory assessment of acid-base status that is needed to formally diagnose DKA. Blood ketones measured with a fingerprick blood sample and appropriate meter can be used to provide an objective measure of DKA risk and severity and can also accurately guide management (Figure 2).17 We highly recommend that patients with type 1 diabetes obtain a blood glucose meter that is capable of measuring blood ketones. Ketone levels greater than 1.5 mmol/L indicate an increased risk of DKA, even if blood glucose levels are not markedly elevated. Serum glucose concentration does not correlate well with blood ketone concentration because the rates of glucose and ketone production and use are not the same at different stages of DKA. Severe ketosis can be missed if it is not investigated until severe hyperglycaemia is also present.
{kind=link}
The decision to send patients with positive ketones for assessment in the emergency department will depend on clinical status and their ability to follow a management plan during a minor intercurrent illness (a sick day management plan), which should consist of a written plan on frequency of monitoring, additional insulin administration and increased fluid intake. Patients who are unable to correct mild ketosis, who have a ketone level of 0.6 mmol/L or more that is not decreasing with supplemental insulin, or who have a level greater than 1.5 mmol/L should be sent to hospital for assessment and treatment.18,19
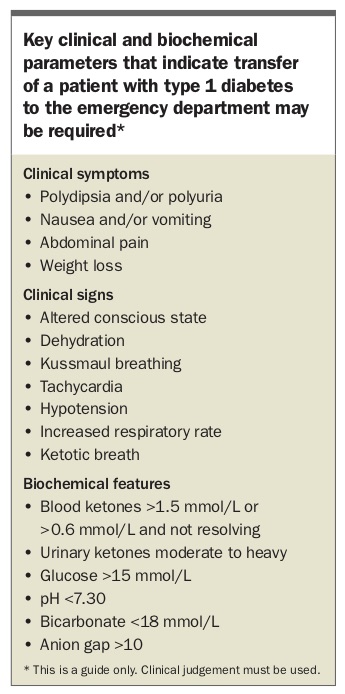
DKA is an endocrine emergency and if patients present with haemodynamic instability, clinical signs of severe dehydration or neurological symptoms, prompt referral to a hospital is warranted. If in doubt, patients should be referred to an emergency department or advice from a diabetes specialist should be sought (Box). The recent RACGP and Australian Diabetes Society joint clinical position statement on emergency management of hyperglycaemia in primary care provides valuable information (www.racgp.org. au/download/Documents/Guidelines/Management-of-hyperglycaemia.pdf).20
{kind=link}
Management of DKA in hospital
Management of DKA in hospital should follow international or local guidelines. Overall, it is accepted that fluid and potassium replacement are the most important initial therapeutic interventions followed by insulin administration. However, guidelines differ in recommendations for choice of fluids and route and rate of insulin administration.21
The fluid deficit in patients with DKA may be severe and up to 10% of total body weight.1 Isotonic and crystalloid solutions have been the preferred fluid choice. There is very weak evidence for using balanced electrolyte solutions to reduce the risk of hyperchloraemic metabolic acidosis.21 Major guidelines recommend fluid replacement with crystalloid fluids with addition of glucose solutions at variable speed and concentration once the blood glucose level falls. Addition of glucose is important since blood glucose levels may decrease rapidly as ketoacidosis improves and resultant hypoglycaemia may result in rebound ketosis.1,5
Patients with DKA usually present with high-normal or elevated serum potassium due to acid exchange; however, importantly they have a total body potassium deficit.22 Initiation of insulin causes a shift of potassium back into the cellular compartment, which could precipitously lower the serum potassium concentration, potentially causing fatal cardiac arrhythmias. Careful potassium replacement even in patients with high-normal potassium levels at presentation, regular potassium measurements and, in some cases, cardiac monitoring are crucial. Different trials and previous publications suggest a range of potassium replacement rates from 10 to 40mmol/hour depending on serum potassium levels.21
The use of intravenous bicarbonate or phosphate is not routinely recommended and significant controversy surrounds phosphate and bicarbonate replacement in DKA. Phosphate can be given cautiously if there is clinical evidence of respiratory or skeletal muscle weakness and levels are markedly decreased (less than 0.4 mmol/L).1,21 Bicarbonate administration should only be considered if the pH is less than 6.9 as there has been evidence it may lead to decreased oxygen uptake in tissues and increase the risk of cerebral oedema and hypokalaemia.21
Once hypokalaemia is corrected and hydration initiated, insulin is administered. The current mainstay is continuous, intravenous therapy with regular insulin. Evidence supports continuation of the patient’s long-acting subcutaneous insulin to prevent rebound hyperglycaemia when intravenous infusions are discontinued after resolution of DKA.21 Major guidelines suggest a fixed-rate intravenous insulin infusion of 0.1 units/kg with adjustment of rates depending on blood glucose levels.1,5
Measuring blood glucose hourly, ketones second-hourly and electrolytes fourth-hourly and intensive monitoring of vital signs is recommended. Most hospitals in Australia will have ketone meters available but, if not, the rate of increase of bicarbonate levels and decrease in blood glucose levels and normalisation of anion gap are alternative measures.6 The potential underlying causes of DKA need to be investigated and treated. Transitioning to subcutaneous regimens is recommended once resolution of DKA is achieved. An overlap of one to two hours between discontinuation of intravenous insulin and administration of subcutaneous insulin is recommended.5,23
The optimal rate of resolution for the metabolic derangements that characterise DKA remains to be defined, but intensive early correction of hyperglycaemia is associated with a higher rate of adverse outcomes compared with partial early correction.24
In one Australian hospital with their own DKA protocol, a mean time to resolution of acidosis of 11 hours was found.11 Research at the Townsville Hospital in Queensland showed that patients managed with a local protocol had a shorter mean time to normalisation of serum bicarbonate, a lower incidence of hypokalaemia and hypoglycaemia, no significant difference in total insulin dose and a shorter duration of hospitalisation.10 This led to the development and implementation of a Queensland-wide DKA protocol.17
Similarly to other major protocols, it emphasises fluid and electrolyte replacement followed by insulin administration.17 The four-page document outlines when to suspect and how to diagnose DKA and gives a step-by-step approach to fluid, electrolyte and insulin administration. It also outlines investigations that should be considered for possible underlying causes of DKA. It emphasises the need to replace and monitor serum potassium levels and recommends early escalation of care to an intensive care unit in the presence of any of the following:
- venous pH of less than 7.1
- severe hypokalaemia (serum potassium level <3 mmol/L)
- severe hyponatraemia (serum sodium level <125 mmol/L)
- severe dehydration
- cardiorespiratory compromise
- pregnancy
- signs of altered level of consciousness.17
A strong warning to monitor closely for signs of cerebral oedema is also included.
This protocol is routinely used in emergency departments and inpatient wards throughout Queensland. The full version can be downloaded from www.health.qld.gov.au/__data/assets/pdf_file/0028/438391/ diabetic-ketoacidosis.pdf. Protocols are guides only and are no substitute for clinical judgement and individualised patient care.
Prevention
It is important that diabetes experts are involved in the care of patients with DKA to provide strategies to prevent further episodes. Many cases of DKA can be avoided by education and improved follow-up care. Patients should receive a written sick day management plan with instructions on how to adjust insulin during illness, with an emphasis on how to manage persistent hyperglycaemia, continuation of long-acting insulin and the need to increase fluid intake. They should receive education on how to monitor blood glucose and ketone levels during illness and the importance of recognising DKA early and seeking prompt medical attention. Practical guidelines for sick day management are available, covering care of children and adolescents (https://cdn.ymaws.com/www.ispad.org/resource/resmgr/Docs/
CPCG_2014_CHAP_13.pdf)18 and care of adults (www.adea.com.au/wp-content/uploads/2009/10/ClinicalGuiding-Principles-for-Sick-Day-Management-of-Adults-with-type-1-and-type-2-diabetes1.pdf).19
Shared care including detailed handovers between GPs and diabetes experts is of utmost importance. Many occurrences of DKA can indicate a failure of care, leading to recurrent hospital admissions. In some people lack of self-care and recurrence of DKA cluster. Targeted clinics for high-risk patients such as hospital avoidance clinics exist and GPs can refer patients to these clinics.25
Conclusion
DKA is a common complication of diabetes and often develops in the outpatient setting. Prompt recognition of DKA, appropriate fluid resuscitation and insulin administration with attention to electrolyte imbalances are of paramount importance. General practitioners play a pivotal role in identification and prevention of this potentially life-threatening complication. ET