New agents to treat type 2 diabetes

Diabetes type 2
Diabetes medicines
The distinct pros and cons of three new classes of type 2 diabetes medication provide many options for individualised, safe treatment. Therapy may now be prescribed based on consideration of factors such as cardiac or renal protection, not only blood glucose lowering.
- In the past 10 years three new classes of diabetes medications have been introduced: the glucagon-like peptide-1 (GLP-1) receptor agonists; dipeptidyl peptidase-4 (DPP-4) inhibitors; and sodium–glucose cotransporter-2 (SGLT-2) inhibitors. None of these agents cause hypoglycaemia when used alone or in combination with metformin.
- GLP-1 receptor agonists have robust glycated haemoglobin- lowering properties and very good weight-reduction potential.
- GLP-1 receptor agonists are administered by injection, which may decrease their acceptability for some patients; exenatide can be given weekly, which may appeal to some patients.
- GLP-1 receptor agonists are not recommended in patients with significant renal disease.
- SGLT-2 inhibitors have many benefits including effective glucose lowering, blood pressure reduction and weight loss, and they have been shown to reduce hospitalisation for heart failure and improve renal outcomes.
- Empagliflozin has been shown to reduce cardiovascular death in patients with type 2 diabetes and prior cardiovascular disease.
- SGLT-2 inhibitors can only be used if the eGFR is adequate (>45 mL/min/1.73m2 for empagliflozin and >60mL/min/1.73m2 for dapagliflozin), and some patients may be unable to take them due to genital mycotic infections, polyuria or postural hypotension.
- DPP-4 inhibitors are a great alternative for patients with impaired renal function or who cannot tolerate other agents.
- DPP-4 inhibitors may offer slightly less glucose-lowering and weight-loss potential than the other new agents.
Picture credit: © BSIP/Diomedia
The number of medications for treating diabetes has expanded rapidly in recent years. The Australian Diabetes Society guidelines for the treatment of type 2 diabetes and the closely associated Royal Australian College of General Practitioners (RACGP) guidelines list eight different classes of medications that can be used in countless combinations.1,2 Furthermore, there are differences within each class that add complexity, and the speed with which new classes and new individual medications have appeared has exacerbated confusion about their appropriate use.
In the past 10 years alone, three new classes have been introduced: the glucagon-like peptide-1 (GLP-1) receptor agonists; dipeptidyl peptidase-4 (DPP-4) inhibitors; and the sodium–glucose cotransporter-2 (SGLT-2) inhibitors. Not all agents that are TGA approved are available on the PBS, and those that are listed on the PBS require streamlined authority to prescribe, based on an ever-changing list of streamlined authority numbers. This review focuses on the clinical use of these new medications in the Australian context.
Glucagon-like peptide-1 receptor agonists
Overview
GLP-1 is an incretin hormone that is secreted by the gut after eating. It has multiple effects including stimulating insulin release, decreasing glucagon secretion, slowing gastric emptying and reducing hunger signals from the hypothalamus. It is broken down within minutes by the enzymatic action of DPP-4, and so analogues to endogenous GLP-1 were developed that are resistant to breakdown by DPP-4 but still have all the beneficial actions of GLP-1.
The first GLP-1 receptor agonists were introduced in 2006 and were the first glucose- lowering medications that could also help to reduce weight (via their actions on the stomach and the brain). One of the available preparations of the GLP-1 receptor agonist exenatide only needs to be administered weekly and is the only diabetes medication with this convenience. On the other hand, GLP-1 receptor agonists are the only class of the newer agents that need to be given by subcutaneous injection. Another GLP-1 receptor agonist, liraglutide, was shown to decrease composite cardiovascular endpoints in a large clinical trial.3
Glycaemic effect
Due to their multiple actions, the GLP-1 receptor agonists effectively reduce both fasting and postprandial glucose levels. They are relatively potent, and reduce glycated haemoglobin (HbA1c) levels by around 1% in most patients.4 Nonresponders do exist, but so far there is no reliable way of predicting a patient’s response other than by trialling the medication.
Side effects
The dual actions of stimulating insulin and suppressing glucagon release would lead to the expectation that GLP-1 receptor agonists may cause hypoglycaemia. However, these effects are glucose dependent. That is, they occur when the plasma glucose is high, but the effects attenuate when the blood glucose levels are in the normal or hypoglycaemic ranges.5 This means that, in reality, the GLP-1 receptor agonists do not increase the risk of hypoglycaemia when used alone or in combination with metformin.
The main adverse effects of the GLP-1 receptor agonists are nausea and vomiting, thought to be a consequence of their action in slowing gastric emptying. This is the most common reason why some patients cannot use a GLP-1 receptor agonist, but this impact can be reduced by a ‘start low, go slow’ dose-titration strategy. The exception to this approach is weekly administered exenatide, as the full 2 mg weekly dose builds plasma levels slowly over about six weeks. Also, there is evidence that nausea decreases over time, so perseverance may overcome the initial problem.
Site reactions can occur and are more common with the weekly exenatide preparation. Pea-sized subcutaneous nodules that persist may also occur with weekly exenatide, due to the volume of the injection and the microsphere technology that prolongs its action.6 Pancreatitis was initially thought to be a problem of GLP-1 receptor agonists, but the large cardiovascular outcome trials have shown that this is not a clinically significant problem.3
PBS indications
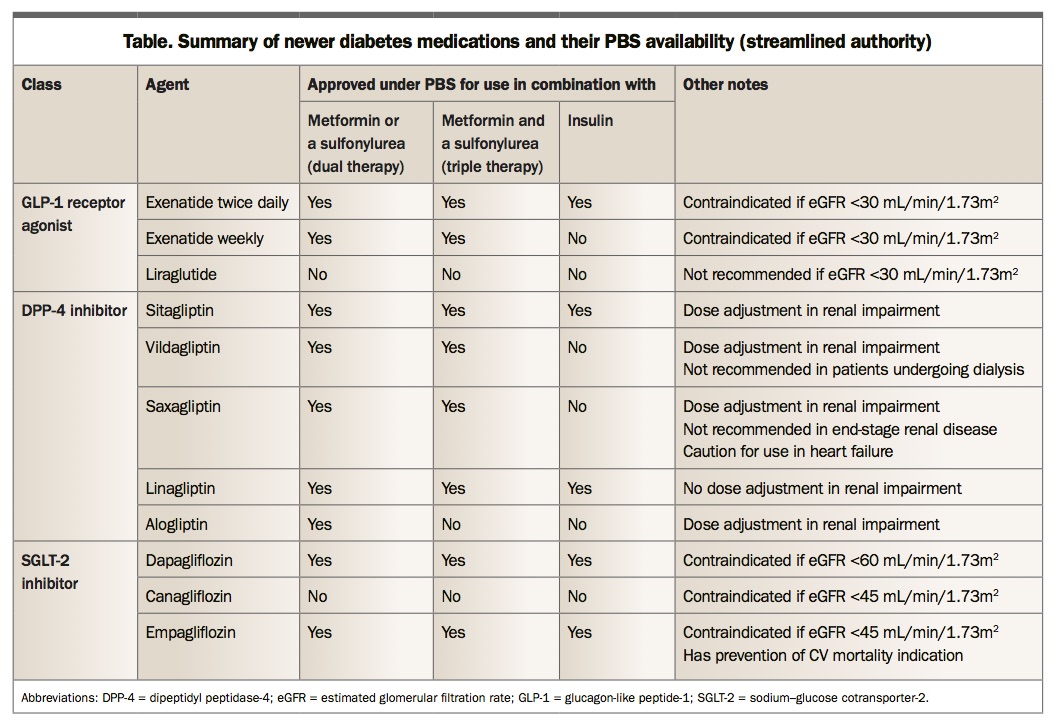
Exenatide twice-daily and weekly preparations are approved under the PBS for use in combination with metformin and/or a sulfonylurea. However, only twice-daily exenatide is approved for use with insulin. Liraglutide is not currently listed on the PBS.
Use of exenatide in combination with DPP-4 inhibitors, SGLT-2 inhibitors and thiazolidinediones (TZDs) is contraindicated. In patients with renal impairment, exenatide is contraindicated and liraglutide is not recommended if eGFR is less than 30 mL/min/1.73m2. See the Table for a summary of the PBS streamlined authority indications for these and other medications discussed.
{kind=link}
Place in clinical practice
GLP-1 receptor agonists are ideal for patients with HbA1c levels above target for whom weight loss is a priority and who do not mind having injections. Liraglutide has a specific weight loss indication, even in the absence of diabetes. Additionally, there is evidence that liraglutide is protective against cardiovascular disease.
Some patients prefer weekly therapy with exenatide; however, for those on insulin seeking to minimise weight gain or insulin dose, twice-daily exenatide would be more appropriate. Treatment with a GLP-1 receptor agonist is not suitable for patients with significant renal disease.
Dipeptidyl peptidase-4 inhibitors
Overview
Another way to increase endogenous GLP-1 action is to slow its breakdown by the enzyme DPP-4. The DPP-4 inhibitors do exactly that, prolonging the action of endogenously secreted GLP-1, leading to most of the same incretin-based benefits as the GLP-1 receptor agonist class, such as glucose lowering. Compared with an exogenously administered GLP-1 receptor agonist, they do not increase GLP-1 action as much, and are therefore somewhat less effective; most notably, there is no discernible weight-loss effect. On the other hand, the DPP-4 inhibitors are oral medications. Their main claim to fame is their remarkably benign safety profile (see side effects, below) which means they are the only class of diabetes medication other than insulin that can be used in any degree of renal impairment or failure. Dose adjustment is required in patients with decreased kidney function, except with linagliptin, which can be used at its full 5 mg dose with any eGFR. Fixed-dose combinations of a DPP-4 inhibitor with metformin increase their convenience of use.
Glycaemic effect
The HbA1c-lowering potential of DPP-4 inhibitors in most trials has been shown to be about 0.5%.7,8 This is consistent with the notion that DPP-4 inhibitors are weaker than GLP-1 receptor agonists.
Side effects
The flip side of the reduced incretin effect is that DPP-4 inhibitors are almost free of any adverse effects. Early in the development program, there were concerns regarding nasopharyngitis and pancreatitis, but large outcome trials have shown their safety and tolerability.9-12
There are only two considerations. The first is that saxagliptin was shown to increase the relative risk of hospitalisation with heart failure by about 20% in patients with type 2 diabetes who had a history of cardiovascular events (although the absolute risk increase was less than 1%).10 Alogliptin showed the same trend to a lesser degree, but sitagliptin demonstrated no similar effect.11,12 It is unknown whether linagliptin or vildagliptin affect cardiac failure. Second, vildagliptin can sometimes be associated with raised liver function test results, so these should be periodically monitored in patients taking this drug.
In general, DPP-4 inhibitors cause no side effects in those taking them. They do not increase the risk of hypoglycaemic episodes when used alone or with metformin. They are among the most well tolerated of any prescription medicines. However, multiple cardiovascular outcome studies have demonstrated no specific benefit of drugs in this class over alternative traditional therapies.
PBS indications
All DPP-4 inhibitors are currently PBS approved for use in combination with metformin or a sulfonylurea, and all except alogliptin have PBS approval for triple therapy with metformin and a sulfonylurea. Sitagliptin and linagliptin are also PBS-approved for use with insulin. Combinations with GLP-1 receptor agonists, SGLT-2 inhibitors and TZDs are excluded.
Place in clinical practice
DPP-4 inhibitors have a place for use in patients in whom other options may be problematic, whether due to pre-existing renal disease or other side effects. This is especially pertinent in elderly populations, and DPP-4 inhibitors are regarded as the preferred therapy in this vulnerable group, particularly if there is no specific clinical indication for cardiovascular risk prevention.
Once-daily oral administration as well as fixed-dose combinations with metformin add to their convenience of use. Sitagliptin and linagliptin can be added to insulin to either improve glucose control or help reduce insulin dose. Conversely, they offer slightly less potential for lowering HbA1c and weight compared with the GLP-1 receptor agonists or SGLT-2 inhibitors.
Sodium-glucose cotransporter-2 inhibitors
Overview
The most recent addition, this class of medications offers great benefits but also requires some caution in their use. The SGLT-2 inhibitors block the resorption of glucose in the proximal convoluted tubule of the kidney.13 This directly results in glucose being eliminated via the urine (thus lowering plasma glucose) and delivers more sodium to the distal tubule (leading to a mild diuretic/natriuretic effect). These actions, respectively, account for the additional benefits of weight loss and blood pressure lowering among patients taking SGLT-2 inhibitors.
Perhaps even more significantly, large randomised controlled outcome trials have demonstrated a reduction in composite cardiovascular events among patients with established cardiovascular disease taking empagliflozin or canagliflozin.14,15 Additionally, both studies showed protection against hospitalisation for heart failure and progression of renal disease. The decrease in cardiovascular death was so robust for empagliflozin that it has TGA approval for use in patients with type 2 diabetes and prior cardiovascular disease. Prevention of cardiovascular death is currently a unique indication for any diabetes medication. However, it is uncertain whether these benefits, which are probably not mediated by glucose lowering, extend to patients with type 2 diabetes without established cardiovascular disease.
Glycaemic effect
Most studies of SGLT-2 inhibitors show HbA1c lowering of about 0.7% when the starting HbA1c is below 9%.16 This is fairly consistent as long as the patient’s renal function is relatively normal (because glucose lowering is dependent on the kidneys being able to filter glucose).
These agents become less effective for glucose lowering at lower levels of renal function. Thus, dapagliflozin is contraindicated if the patient’s eGFR is less than 60 mL/min/1.73 m2, and empagliflozin and canagliflozin are contraindicated if the eGFR is less than 45 mL/min/1.73 m2. However, the blood pressure and cardioprotective effects of empagliflozin seem to be maintained with an eGFR as low as 30 to 45 mL/min/1.73 m2. There is also evidence that the higher the patient’s initial HbA1c level, the greater the glucose-lowering effect, because glomerular glucose filtration is also dependent on plasma glucose concentration.
Side effects
The most common adverse reactions in patients taking SGLT-2 inhibitors are genital fungal infections, which occur at about five times the baseline rates for both men and women. Interestingly, the risk of urinary tract infections is only slightly increased.14,15 Osmotic diuresis may lead to polyuria, or even postural hypotension.
More concerningly, there is a slight increase in diabetic ketoacidosis.17 While this is mainly seen when these medications are used in patients with type 1 diabetes, it can also occur in patients with type 2 diabetes. The particular feature of the diabetic ketoacidosis caused by SGLT-2 inhibitors is that it can be euglycaemic; that is, the blood glucose is often below 10 mmol/L when it develops. The practical implication is that patients who develop vomiting or other general illness while on SGLT-2 inhibitors should be tested for the presence of ketones even if the blood glucose is in or near the normal range.
The large outcome studies showed other interesting side effects. Canagliflozin significantly increased the risk of lower limb amputation and fractures.15 These effects were not seen in the empagliflozin study, and it is not clear whether these are class effects or are issues peculiar to canagliflozin. Empagliflozin was associated with a small nonsignificant trend towards increased stroke events.18
PBS indications
Empagliflozin and dapagliflozin have streamlined PBS authority approvals for use with metformin and/or a sulfonylurea and with insulin in patients with type 2 diabetes. Combinations with a TZD, a DPP-4 inhibitor or a GLP-1 receptor agonist are disallowed under the PBS. Canagliflozin is not currently on the PBS.
Place in clinical practice
Overall, once-daily oral administration makes SGLT-2 inhibitors a convenient choice for those who can tolerate them and who might benefit from the robust glucose lowering, weight loss and blood-pressure lowering provided by this new class of medications. Additional evidence supports improved cardiovascular outcomes and renal protection with empagliflozin and canagliflozin. Fixed-dose combinations with metformin are also available to reduce pill burden.
Nevertheless, despite the multitude of benefits, SGLT-2 inhibitors are not appropriate for every patient. The most common contraindication is a low eGFR, with the limits noted above. In general, patients with a preserved eGFR would be more suited to using an SGLT-2 inhibitor, while those with an eGFR less than 45 mL/min may be better off taking a DPP-4 inhibitor or GLP-1 receptor agonist (if eGFR is greater than 30 mL/min/1.73 m2). Note that it is not dangerous to use SGLT-2 inhibitors in patients with a low eGFR, but in this setting they are less effective in lowering blood glucose.
Other side effects prevent general use of SGLT-2 inhibitors in all patients with type 2 diabetes, even in patients with adequate renal function. Genital fungal infections are usually minor and easily treatable, but SGLT-2 inhibitors should be ceased in those with recurrent episodes. Polyuria and hypotension are uncommon, but caution should be exercised in patients taking loop diuretics and those at high falls risk. Euglycaemic diabetic ketoacidosis is rare and is not of great concern in patients with type 2 diabetes, but SGLT-2 inhibitors should be avoided in patients with type 1 diabetes. The clinical significance of the increased amputation and fracture rates with canagliflozin are still uncertain.
Conclusion
We are now moving into an era where choice of type 2 diabetes therapy may be driven by reduction of cardiovascular and mortality risk rather than purely on glucose-lowering effects. In this regard, SGLT-2 inhibitors and some GLP-1 receptor agonists may have a role, particularly in patients with established cardiovascular disease. Common traits of the new agents are that they carry a low risk of hypoglycaemia and do not cause weight gain, which often gives them the edge over the traditional second- and third-line medications, sulfonylureas and insulin, despite increased cost compared with sulfonylureas. They have distinct advantages and disadvantages, so individualised treatment is a consideration. Patients with impaired renal function are best treated with DPP-4 inhibitors. SGLT-2 inhibitors are for those with no significant history of renal impairment or genital thrush, but who might benefit from weight loss or cardiovascular risk reduction. Lastly, the GLP-1 receptor agonists can be used in patients who do not mind an injection, would like to lose weight, may prefer a weekly treatment and also have near normal renal function. ET