The driver with diabetes: a guide to assessment and reporting

Impaired driving
Diabetes complications
The driver with diabetes, their healthcare professionals and the relevant driving licensing authority each have roles and responsibilities in helping to minimise health-related road crashes, serious injuries, and emotional and economic costs. This article explores fitness to drive in people with diabetes in light of contemporary national guidelines and requirements.
- The main health-related driving concern in people with diabetes treated with glucose-lowering medications is the occurrence of a severe hypoglycaemic event while driving, potentiating a crash risk.
- Impaired vision, neuropathy, sleep disorders and cardiovascular disease are significant diabetes complications and related comorbidities that require assessment as they may also affect fitness to drive.
- The Assessing Fitness to Drive publication provides helpful advice to healthcare professionals, including mandatory requirements in the assessment process.
- To help minimise the occurrence of hypoglycaemia while driving, a person taking glucose-lowering medications should ensure their blood glucose level is above 5.0 mmol/L before driving.
- Occurrence of a severe hypoglycaemic event in a person with diabetes requires cessation of driving, and a nondriving period with a comprehensive reassessment by the relevant medical healthcare team.
Picture credit: © Tyler Olson/adobe.com Model used for illustrative purposes only.
In Australia in 2016 there were 17.2 million drivers on the road, and based on self-reported data in 2014-15 an estimated 1.2 million adults in Australia (6%) have diabetes.1,2 The Australian 2016 publication on Assessing Fitness to Drive (AFTD) includes a diabetes-specific section (pages 59 to 66), which forms a foundation for this article addressing diabetes and driving.3
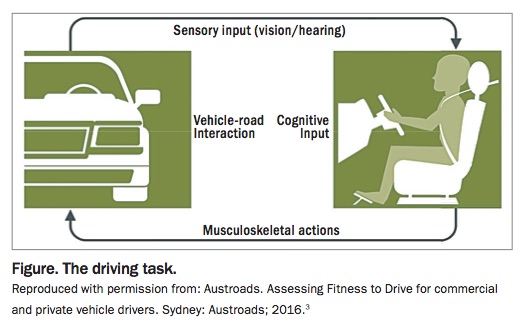
The AFTD publication provides guidance to healthcare professionals and state- and territory-based driver licensing authorities (DLAs) in making licensing decisions in individuals based on consideration of the driving task (Figure). The driving task requires a level of skill and ability to interact with the vehicle and external environment at the same time, and depends on biological functions such as sensory input (e.g. vision and proprioception), cognitive function (e.g. concentration, judgement, decision making) and motor function (e.g. co-ordination).
{kind=link}
In drivers who have diabetes, the most significant concern is the occurrence and impact of a severe hypoglycaemic event while driving. Findings point to a higher crash risk in people with a history of severe hypoglycaemia. There is also evidence that tighter control, as measured by HbA1c, may be associated with an increased risk of a motor vehicle crash.4
The purpose of the AFTD standards is to help optimise road safety in Australia by assisting healthcare professionals to:
- assess fitness to drive in their patients in a consistent and appropriate manner based on current medical evidence and to make recommendations regarding conditional licenses
- promote responsible behaviour in their patients in regard to their medical fitness to drive
- recognise the extent and limits of their professional and legal obligations with respect to reporting fitness to drive.
Assessment and reporting on fitness to drive
There are two sets of medical standards for driving licensing or authorisation, which are private and commercial vehicle driver standards. Commercial vehicle standards thresholds and requirements are generally higher than those for private standards. A conditional licence application is often required in a person with diabetes if they are treated with a glucose-lowering medication, especially insulin. A conditional licence identifies the need for medical treatments, vehicle modifications and/or driving restrictions to enable the person to drive safely. Specified medical review periods are also required to establish the status of diabetes and continued fitness to drive.
Assessing and reporting on fitness to drive is outlined in a step-by-step process including determining the type of licence held or under application and undertaking a clinical examination in conjunction with the patient’s medical history, driving history and driving needs in the AFTD publication on pages 26 to 32.
Key roles and responsibilities
Driver with diabetes
Key roles and responsibilities of the driver with diabetes are to:
- report to the DLA a permanent condition such as diabetes that may affect their ability to drive safely
- respond truthfully to questions from healthcare professionals and the DLA
- adhere to prescribed medical treatment
- comply with the requirements of a conditional licence as appropriate.
Healthcare professionals
Key roles and responsibilities of healthcare professionals in ensuring fitness to drive are to:
- assess the person with diabetes for fitness to drive based on relevant clinical and functional information and on the relevant published medical standards
- advise the person with diabetes regarding the impact of their medical condition on their ability to drive, any restrictions and ongoing monitoring as required
- be responsible for advising the DLA regarding a person with diabetes of their fitness to drive including their ongoing
- suitability to hold a conditional licence
- provide a letter or notification if a patient’s medical condition improves to such an extent that the licence restriction may be reconsidered by the DLA, resulting in reinstatement of the licence or removal or variation of licence conditions.
Driver licensing authority
Key roles and responsibilities of the DLA are to:
- make all final decisions regarding the licensing of drivers with diabetes
- make all final decisions regarding the issuing of conditional licences in people with diabetes
- educate the driving public with diabetes of their responsibility to report any long-term condition.
Hypoglycaemia
Definition of a severe hypoglycaemic event
Any person treated with insulin and/or other glucose-lowering medications (e.g. sulfonylureas) is at risk of experiencing a severe hypoglycaemic event. During a severe hypoglycaemic event, a person is unable to self-treat the hypoglycaemia and requires an outside party to give immediate treatment, which could include a glucagon injection. Severe hypoglycaemia, which could occur at any time of the day or night, may cause confusion, delayed reaction speed, reduced sensorium and loss of consciousness or a seizure. Impairment of consciousness and judgement can develop rapidly during severe hypoglycaemia and result in loss of control of a vehicle. Experiencing severe hypoglycaemia while driving is thus particularly significant in that brain dysfunction may affect perception, motor skills and changes in behaviour, and it may impair the ability of the person to drive, leading to a motor vehicle crash.
What to do if a severe hypoglycaemic event occurs
If a severe hypoglycaemic event occurs at any time, whether it is during driving or not, the person must not drive for a substantive period of time, which is generally a minimum period of six weeks. Prompt assessment by a healthcare professional with a discussion of the person’s driving history, glucose patterns, behaviour changes and the resolution of any impaired hypoglycaemia awareness should take place. The patient should also document prospective blood glucose levels regularly and improve behavioural cues to minimise the risk of severe hypoglycaemia recurring. The patient should be assessed by an endocrinologist or a diabetes physician, and possibly also by a diabetes educator and/or dietitian.
A severe hypoglycaemic event is less common than mild/nonsevere hypoglycaemia, of which the latter can be self-treated and exhibits a spectrum of autonomic symptoms including sweating, tremor, hunger, headache and palpitation. This nonsevere hypoglycaemic event will not place the driver at immediate risk of a motor vehicle crash but it does indicate the need for prompt treatment to avert severe hypoglycaemia and sequelae.
Causes of hypoglycaemia
Hypoglycaemia may be precipitated by factors including combinations of taking too much insulin for the amount of carbohydrate intake (‘insulin to carb mismatch’), incorrect dosing of other noninsulin glucose-lowering medications (such as sulfonylureas) changes to usual meal patterns, unexpected exertion, any alcohol intake or a combination of these factors. Meal regularity and adjustment in diabetes medication are important discussion points, especially for people who drive long distances or are shift workers. In addition, excessively tight control of blood glucose levels may also increase the risk of hypoglycaemia.
Reduced or impaired awareness of hypoglycaemia
Reduced or impaired awareness of hypoglycaemia is an important, common condition in people with diabetes. It increases the risk of a severe hypoglycaemic event occurring and can be recognised when a person does not regularly sense the usual early warning (autonomic) symptoms of hypoglycaemia. The autonomic symptoms are usually experienced when blood glucose levels are in the 3 to 4 mmol/L range. Impaired awareness of hypoglycaemia can also be identified when a person does not experience hypoglycaemia symptoms until blood glucose levels are below 3 mmol/L, and then these are often only the neuroglycopenic symptoms (e.g. concentration difficulty, behaviour change, weakness, tiredness, confusion, reduced level of consciousness and inability to self-treat hypoglycaemia).
A long duration of diabetes (at least 10 years) or severe hypoglycaemia occurrence markedly increases the risk of impaired awareness of hypoglycaemia. In turn, impaired awareness of hypoglycaemic markedly increases the risk of a severe hypoglycaemia event occurring by three- to six-fold. Impaired awareness of hypoglycaemia therefore poses a risk for road safety.5 Use of the eight-question Clarke hypoglycaemia awareness questionnaire (page 61 of the AFTD publication) may be helpful to assess for impaired awareness of hypoglycaemia, especially in patients taking insulin who have had diabetes for many years and/or following a severe hypoglycaemic event. Four or more ‘R’ responses in the questionnaire implies reduced awareness.6,7 People with type 1 diabetes are most at risk of impaired awareness of hypoglycaemia, in whom it occurs in one-quarter to one-third of patients. Hypoglycaemia awareness can often be improved over weeks or months by avoidance of hypoglycaemia following a severe hypoglycaemic episode.5
A person with persistent impaired awareness of hypoglycaemia should ideally be under the care of an endocrinologist, a diabetes physician and/or a diabetes nurse practitioner with expert knowledge in managing diabetes and who ideally should be involved in assessing their fitness to drive. Any driver who has a persistent impaired awareness of hypoglycaemia is generally not fit to drive commercial vehicles unless their early warning symptoms return.
Acute hyperglycaemia
Drivers with diabetes should receive specific advice about management of their diabetes when they are unwell. They should be advised to follow their sick day plan and to not drive if acutely unwell with unstable diabetes.
Gestational diabetes
Temporary conditions such as gestational diabetes do not impact licensing; however, women who require insulin should be educated to recognise and treat hypoglycaemia symptoms if they occur.
Diabetes comorbidities and complications that may affect driving
Vision
Visual acuity should be measured for each eye separately and without optical correction. If optical correction is needed, vision should be retested with appropriate corrective lenses. Retinal screening should be undertaken every second year if there is no retinopathy, or more frequently if retinopathy is present. Visual field testing is also required in some states and territories and at any time that it is clinically indicated.
Neuropathy and foot care
Drivers with functional problems that are likely to result in difficulty undertaking the driving task need to be identified. Functional problems include the presence of severe neuropathy and inadequate sensation and leg and foot movement for the operation of foot controls. Several small comparison studies in people with type 2 diabetes with lower extremity severe neuropathy have shown delayed brake response times.8
A person with peripheral neuropathy that significantly impairs muscle power, sensation or co-ordination is unable to hold a commercial licence. In some cases, following an individualised assessment, cars can be converted from foot control pedals to hand controls to enable a person with dense lower limb neuropathy to drive.
Sleep apnoea
Sleep apnoea is present on overnight monitoring in 9% of adult women and 24% of adult men, and some studies also suggest there is a higher prevalence of sleep apnoea in long distance vehicle drivers.9,10
Sleep apnoea is also positively associated with type 2 diabetes and difficult to control hypertension. Common clinical features of sleep apnoea include onset of sleep while actively performing tasks, snoring during sleep and witnessed apnoeic events by partners (e.g. often while sleeping, watching television, reading, travelling in a car). Physical features include obesity with a body mass index greater than 35 kg/m2, a thick neck and a narrow oedematous oropharynx. Sleep apnoea is a common morbidity affecting many people with type 2 diabetes and it has major implications for driving. Uncontrolled sleep apnoea increases the risk of a crash occurring by approximately fourfold, whereas treatment of sleep apnoea appears to negate that risk.11
Cardiac risk factors and symptoms
There are no diabetes-specific medical standards for cardiovascular risk factors and driver licensing. Consistent with good medical practice, people with diabetes should have their reversible cardiovascular risk factors periodically assessed and treated as required. People with new onset cardiac symptoms, such as chest pain or exertional dyspnoea, should have prompt assessment by a cardiologist.
General assessment and management of diabetes and driving
General assessment and management of diabetes in relation to fitness to drive is summarised in the Flowchart. For both private and commercial purposes there are three main treatment-related categories for people with diabetes: those controlled by diet and exercise alone; those being treated with glucose-lowering agents other than insulin; and those treated with insulin. A specialist should be an endocrinologist or consulting physician specialising in diabetes, whereas a treating doctor is generally the patient’s GP. If access to a specialist is difficult, telemedicine such as videoconferencing is encouraged as a means of facilitating access to specialist opinion.
Planning ahead in drivers with diabetes
People with diabetes should be encouraged to make a driving licence review appointment at least six weeks before their renewal date. This allows usual investigations (e.g. blood tests, eye examinations, foot checks, which may include a podiatry report, and review of diabetes self-care) to be arranged. A further appointment may be needed to discuss results and completion of the medical report. Online patient appointment bookings could also incorporate a driving and diabetes category, which may be a useful way of collating information and promoting safe driving in people with diabetes.
To plan ahead in drivers with diabetes, the treating doctor can:
- assess all hypoglycaemic events, contributing factors, usual treatment and glucose supplies on their person and in their motor vehicle
- review use of glucose meters including the record book and/or downloading glucose results and usual arrangements for a
- glucose meter, strips and finger-prick test supplies in the vehicle
- assess insulin self-management practices and advise commercial drivers who are taking insulin that at least three months of structured and documented blood glucose results should be reviewed as part of their annual assessment of fitness to drive; a review with a diabetes educator may be helpful in this case
- enquire about eating habits and regularity, and review if assessment by a dietitian is needed
- enquire if diabetes identification is carried on the patient or at least in their vehicle
- inform all staff including reception staff about the importance of this appointment and the potential related issues (e.g. urgency in completing a driving notification form) which may also reduce potential hostility and demonstrate sensitivity to the needs of the patient.
Educational advice for the driver with diabetes
Educational advice from the national diabetes services scheme on diabetes and driving is available online (see Box). Educational advice for drivers with diabetes includes:
{kind=link}
- considering safety of passengers, other road users and themselves
- undertaking the general medical review requirements as requested by the GP or specialist including arranging
- appointments in a timely manner
- avoiding hypoglycaemia
- not driving if their blood glucose level is at or less than 5.0 mmol/L
- not driving for more than two hours without considering having a snack
- not delaying or missing a main meal
- self-monitoring blood glucose levels before driving and every two hours during a journey
- carrying a fast-acting carbohydrate (or sweet drink) in the vehicle for adequate treatment of hypoglycaemia at all times
- treating mild hypoglycaemia if symptoms occur while driving by:
Conclusion
Diabetes and driving raises the concern of a severe hypoglycaemic event while driving, potentiating a crash risk. Significant diabetes comorbidities and related complications (such as impaired vision, neuropathy, cardiovascular disease and sleep apnoea) may also affect a patient’s fitness to drive and require assessment. Healthcare professionals can help to ensure safe driving for people with diabetes, their passengers and other road users. ET
References
2. Australian Institute of Health and Welfare (AIHW). Australia’s health 2016. Australia’s health no. 15. Cat. No. AUS 199. Canberra: AIHW; 2016. Available online at: https://www.aihw.gov.au/reports/australias-health/australias-health-2016/contents/summary (accessed October 2017).
3. Austroads. Assessing fitness to drive for commercial and private vehicle drivers: medical standards for licensing and clinical management guidelines. Sydney, Austroads; 2016.
4. Redelmeier DA, Kenshole AB, Ray JG. Motor vehicle crashes in diabetic patients with tight glycemic control: a population-based case control analysis. PLoS Med 2009; 6: e1000192.
5. O’Neal D, Jenkins A. Lack of hypoglycaemia awareness in diabetes: why it matters in clinical care. Med Today 2014; 3(5): 27-30.
6. Clarke WL, Cox DJ, Gonder-Frederick LA, Julian D, Schlundt D, Polonsky W. Reduced awareness of hypoglycemia in adults with IDDM. A prospective study of hypoglycemic frequency and associated symptoms. Diabetes Care 1995: 18: 517-522.