Hypertension: practical implications of the new National Heart Foundation guidelines

Hypertension
Heart diseases
The 2016 National Heart Foundation guidelines for diagnosis and management of hypertension in adults address primary and secondary prevention. They target absolute cardiovascular risk and focus on contemporary management of hypertension in the context of an ageing population.
- Validated, regularly maintained, nonmercury sphygmomanometers are recommended for blood pressure (BP) measurement.
- Out-of-clinic BP measurement using home or 24-hour ambulatory measurement is a stronger predictor of outcome than clinic BP measurement.
- Automated clinic BP measurement provides similar readings to home and ambulatory BP measurement, and results are generally lower than those from conventional clinic BP measurement.
- BP-lowering therapy is beneficial (i.e. resulting in reduced stroke, cardiovascular death and all-cause mortality) for patients with uncomplicated mild hypertension.
- For patients with at least moderate cardiovascular risk, lower systolic BP targets of less than 120 mmHg (using automated clinic BP measurement) provide benefit with some increase in treatment-related adverse effects.
- Selection of a BP target should be based on informed, shared decision making between patients and health care providers, considering the benefits and harms, and reviewed on an ongoing basis.
Picture credit: © Image Source/HBSS/Diomedia.com Model used for illustrative purposes only
Hypertension, defined as office-measured blood pressure (BP) of 140/90 mmHg or more, is an independent risk factor for myocardial infarction, haemorrhagic and ischaemic stroke, chronic kidney disease, heart failure and premature death. Lowering BP is one of the most effective means of reducing cardiovascular morbidity and mortality.1,2 As of 2013, hypertension was estimated to affect 6 million Australians over the age of 18 years, equating to a prevalence of 34% in adults. Importantly, about 68% of patients with hypertension have either untreated or uncontrolled hypertension.3 Hypertension is also highly prevalent in the Aboriginal and Torres Strait Islander populations.4 It is clearly established that reducing BP significantly reduces cardiovascular morbidity and mortality among people with hypertension,5-8 including in people with mild hypertension (systolic BP [SBP] 140 to 159 mmHg and/or diastolic BP [DBP] 90 to 99 mmHg).9
Blood pressure measurement and diagnostic criteria
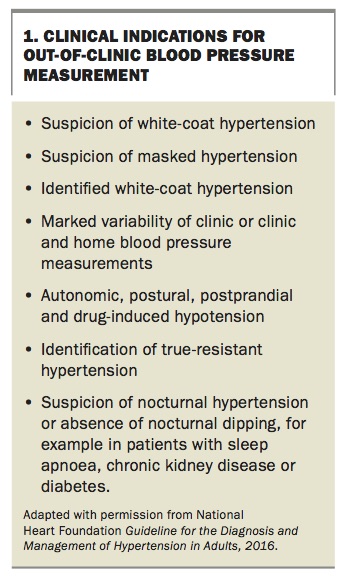
Measurements can be done in the clinic, or out of the clinic with ambulatory BP monitoring (ABPM) or home BP monitoring (HBPM). Out-of-clinic assessments overcome several potential shortcomings of clinic measurements and are useful in several scenarios (Box 1). There is compelling evidence that HBPM, while comparably predictive of cardiovascular events, is better at predicting all-cause and cardiovascular mortality than clinic measurements.10,11 ABPM appears to be better than clinic measurement and HBPM in predicting risk.12 International guidelines, including the United States Preventive Services Task Force and United Kingdom 2011 NICE clinical guidelines13 recommend ABPM as a cost-effective diagnostic technique for all patients with suspected hypertension.
{kind=link}
The 2016 Australian National Heart Foundation (NHF) guidelines14 highlight the relevance and advantages of ABPM, provide clear guidance on its use in clinical practice, and discuss considerations when reviewing and interpreting ABPM data. There is increasing appreciation of the importance of measuring night-time ambulatory SBP. Patients with elevated night-time SBP (‘nondippers’) are at increased cardiovascular risk, even if they are normotensive according to the mean 24-hour ABPM criteria.15 It is important to note that clinic BP measurements are recommended for use in cardiovascular disease risk calculators, because use of HBPM or ABPM may inappropriately underestimate cardiovascular disease risk.
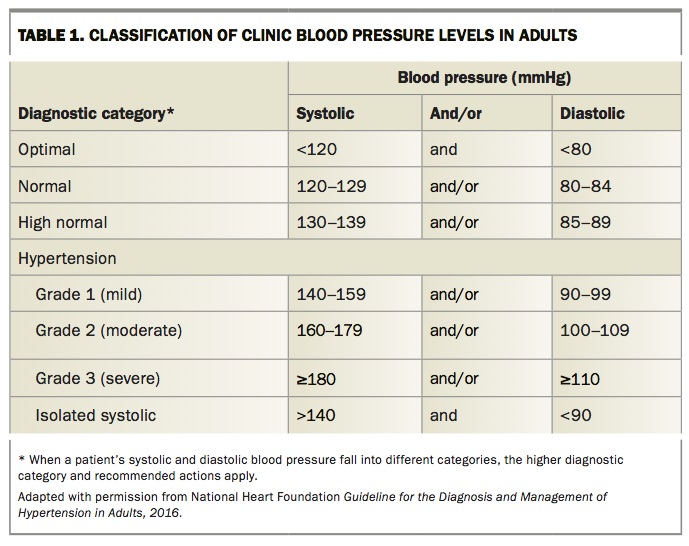
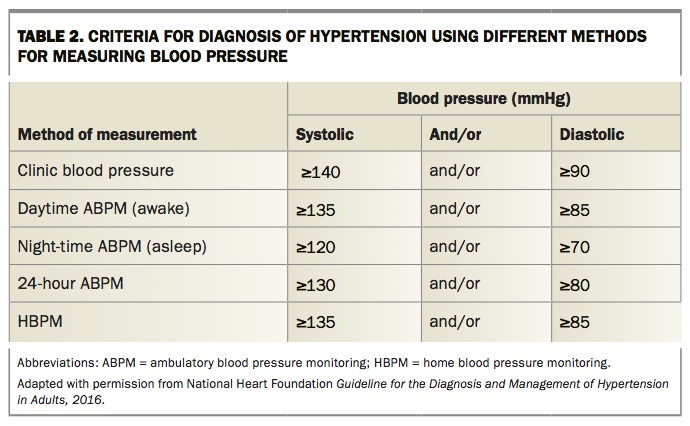
Table 1 summarises the current classification of clinic BP levels (categories) in adults and Table 2 lists the widely accepted diagnostic thresholds for diagnosis of hypertension by the different methods of BP measurement.
{kind=link}
{kind=link}
Whom to treat and targets to use
The benefits of BP reduction are well established across the spectrum of hypertension severity, including in patients with mild hypertension unaccompanied by cardiovascular risk factors.6-10
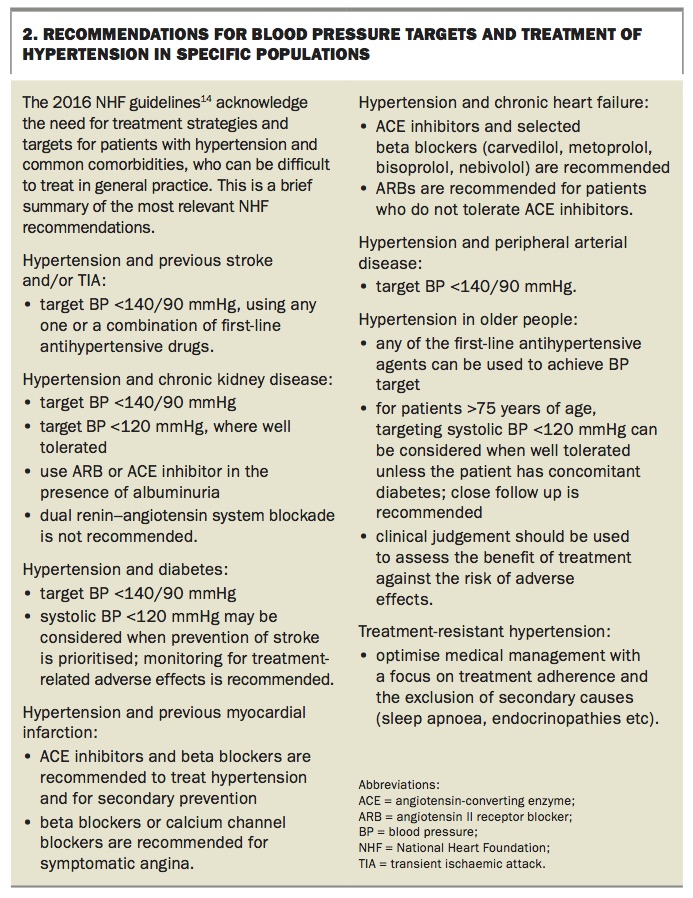
The ideal BP targets for various patient groups remain a matter of debate. However, emerging evidence from randomised controlled trials suggests there is significant benefit from lower BP targets (SBP <120 mmHg) for high-risk populations, including those with previous cardiovascular events, evidence of cardiovascular disease and mild-to-moderate renal impairment.16 The observed benefit is somewhat offset by the higher rates of adverse events (including symptomatic hypotension, syncopal episodes, acute kidney injury and electrolyte disturbances) compared with the rates of adverse events that occur with the standard BP target of less than 140 mmHg. Importantly, the SPRINT trial16 excluded patients with diabetes, which is a significant additive contributor to cardiovascular risk that represents a significant burden in hypertensive populations. The ACCORD trial found that more intense BP reduction in patients with diabetes reduced the risk of stroke, but did not reduce all-cause mortality;17 however, the trial is generally considered to have been underpowered. Meta-analyses suggest that patients with diabetes may also benefit from lower BP targets (<120 mmHg) and this is reflected in the new NHF guidelines (Box 2).
{kind=link}
The conventional BP targets of SBP less than 140 mmHg and DBP less than 90 mmHg are largely unchanged in these new guidelines. They suggest that lower targets (SBP <120 mmHg) in high-risk groups are reasonable if the patient is monitored carefully, given the potential for adverse effects. BP measurements in the SPRINT study were obtained using the principles of automated office BP measurement, that is, the average of three unobserved BP measurements using a semiautomatic device. This method tends to yield a lower BP average than readings obtained with routine clinic BP measurement by doctors or nurses.
First-line agents and combination therapy
Most classes of antihypertensive medicines are equally effective at lowering BP, but fewer than 30% to 50% of patients achieve BP targets with a single agent, so two or more agents are often required for effective treatment. In spite of the five main drug classes being associated with similar cardiovascular mortality, there is evidence of interclass differences in all-cause mortality and cardiovascular events.18 However, a comprehensive review of the literature was conducted for the current guidelines, which recommend that angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs), calcium channel blockers, and thiazide diuretics are suitable first-line drugs.
ACE inhibitors and ARBs are the mostly widely used first-line agents. Their benefits are well established for prevention of cardiovascular events and end organ damage, and there does not appear to be much difference between them except in certain situations. ACE inhibitors are more effective in preventing diabetic nephropathy in early diabetes19 and preventing coronary heart disease in patients with hypertension,20 but ARBs appear to be slightly more effective in preventing kidney failure at more advanced stages of diabetic nephropathy.21 Combining the two drug classes gained significant appeal in the past decade, but this approach has been abandoned and is now deemed contraindicated because of the increased occurrence of adverse outcomes, especially electrolyte disturbances (hyperkalaemia) and renal impairment, without additional benefit.22-24
Calcium channel blockers appear to be especially advantageous over other agents in stroke prevention, as suggested by large meta-analyses.25,26
Certain antihypertensive combinations, in addition to being more efficacious, are judged to be useful in certain situations. Examples include an ACE inhibitor or ARB plus a thiazide diuretic for a patient with heart failure or after a stroke, and an ACE inhibitor or ARB plus a calcium channel blocker for a patient with diabetes and/or a lipid disorder.27 This second combination, ACE inhibitor or ARB plus calcium channel blocker, was found to be superior in reducing overall cardiovascular outcomes in a head-to-head randomised trial enrolling patients with a high risk for cardiovascular events.28
Initiating treatment with combination therapy can be considered if a more rapid achievement of target BP is required,29 and may improve adherence to treatment. However, a direct benefit of this approach on cardiovascular outcomes has not yet been shown. MT
References
https://www.nice.org.uk/guidance/cg127 (accessed November 2017).