Closing the gap in diabetes: how is it going to be achieved?

Diabetes type 2
The growing problem of diabetes is a key contributor to the gaps in health and life expectancy in Indigenous Australians. The causes of the gap are multifactorial and complex, with links to poverty, remoteness and low levels of health literacy and education. Management of diabetes in the Indigenous population requires new, aggressive and innovative management approaches, focusing on primary care resources and new therapies to reduce the burden of complications and disability.
What is the gap?
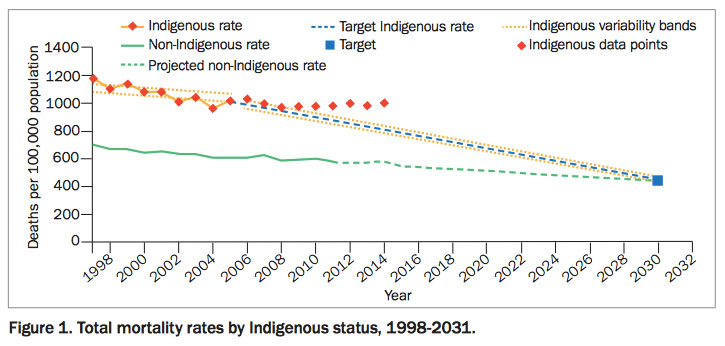
Indigenous health is an issue of national importance and priority. The key areas of disadvantage suffered by the Indigenous population in Australia include gaps in education, employment, health and mortality. The gap in life expectancy between Indigenous and non-Indigenous Australians is unacceptably high (Figure 1). Life expectancy is currently 69 years in Indigenous men and 73 years in women, compared with 79 and 83 years, respectively, in non-Indigenous men and women.1 This gap of about 10 years, which is possibly widening, does not compare well with other international Indigenous populations, including the New Zealand Maori population with a gap of eight years and American Indians with a gap of 4.4 years.2,3
{kind=link}
In 2008, the Council of Australian Governments committed to working towards closing the gap in health and life expectancy in Indigenous Australians by spending $1.6 billion over four years on its Indigenous Chronic Disease Package. The package focused on preventive health, primary healthcare and expansion of the Indigenous work force. Several key strategies and targets were outlined to be achieved over a period of 10 to 20 years. These included halving the gap in childhood mortality, closing the gap in life expectancy, improving education including maximising enrolment in childhood education and improving school attendance and year 12 attainment, and halving the gap in employment.
Key determinants in the gap
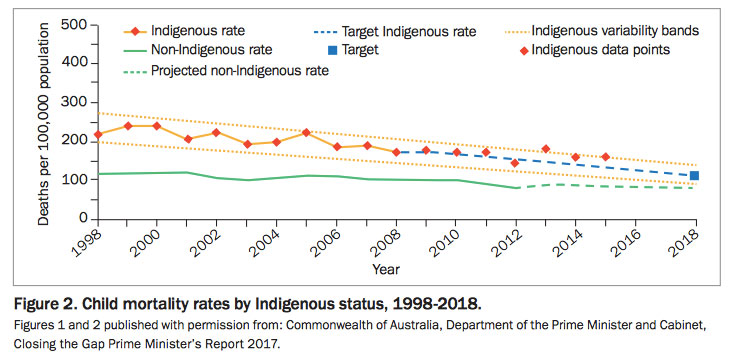
The gap in life expectancy is attributed to a combination of infant mortality, external factors (e.g. accidents, self-harm, assault) and chronic disease. Although infant mortality has fallen significantly, the contribution of chronic disease to excess mortality is increasing. Although the gap in infant mortality has decreased by 64% from 1998 to 2012,4 the target to halve the gap in child mortality by 2018 is not on track this year (Figure 2). The burden of chronic disease continues to increase and contributes to excess mortality, with the leading causes of death being circulatory disease (25%) and neoplasms including cancers (20%). These together with external causes (15%) make up 60% of the mortality in Indigenous populations.4
{kind=link}
Chronic disease and diabetes
Chronic disease accounts for approximately two-thirds of the gap in mortality between Indigenous and non-Indigenous Australians.4 Social determinants such as poverty, poor housing, overcrowded accommodation, poor education, unemployment, substance abuse and remote location contribute to the burden of chronic disease.
Diabetes is one of the leading causes of morbidity and mortality in Indigenous Australians. It is highly prevalent, with 11.1% of Aboriginal and Torres Strait Islander people having diabetes,4 which is about three times the national prevalence. There are many key factors that promote high rates of diabetes, and these are similar in other Indigenous populations around the world. The obesity rate is high at 34% and increasing, and Indigenous people are 1.5 times more likely to be overweight or obese compared with non-Indigenous Australians.5 They are also 1.5 times more likely to be sedentary compared with non-Indigenous people. Many Indigenous people live in remote areas, with 21% of Indigenous Australians living in remote and very remote areas, despite making up only 3% of the population.6 Remote living is associated with reduced access to healthcare services and nutritious food, resulting in increased morbidity and mortality.
Genetics and epigenetics undoubtedly play a significant role in the development of chronic disease and its associated morbidity. Although it is known that diabetes in Indigenous populations occurs earlier and is associated with higher complication rates compared with non-Indigenous populations, the genetics and epigenetics are yet to be clearly defined. It is postulated by some that a ‘thrifty gene’, which was important for maintenance of metabolism and bodyweight in times of food shortage, may be responsible for driving obesity and glucose intolerance in a population that in the 21st century has suddenly experienced dramatic changes to food security and exercise requirements.7
Diabetes-related complications
The burden of complications related to diabetes in Indigenous populations is greater than in non-Indigenous populations. Although there are limited data in many countries including Australia, it is known that all complications, hospitalisation and mortality caused by diabetes are higher in Indigenous people.8
Renal disease is of growing concern in Indigenous populations and this is largely driven by very poorly controlled type 2 diabetes. In Australia, chronic renal disease is present in about 20% of Indigenous people with diabetes, accounting for about 10% of new patients requiring dialysis or transplantation.9 The risk of developing end-stage renal disease in Indigenous people is more than 10 times that of non-Indigenous people.10 The number of people with end-stage renal disease has more than doubled in the past 10 years in Indigenous Australians. Dialysis centres in remote communities are becoming increasingly common and necessary to manage the rapidly growing demands of end-stage renal disease. Death from chronic kidney disease is three times more prevalent in Indigenous compared with non-Indigenous Australians, with the gap in death rates being wider for younger age groups.
Nonproliferative retinopathy is present in 29.4%, neuropathy in 41.2% and cardiovascular disease in 47.1% of Aboriginal Australians with diabetes.11 Mortality due to diabetes is four times that of the non-Indigenous population at 234 deaths per 100,000 compared with 55 per 100,000.12 Hospitalisation rates with type 2 diabetes as the principal or additional diagnosis are four times as high in Indigenous than in non-Indigenous populations.13
What has and is being done to address the gap?
Several reviews on effective interventions and programs, both nationally and internationally, have assessed the key factors associated with improved health outcomes in Indigenous populations. Almost all of these studies point to community involvement and ownership of programs and interventions as being essential and associated with improvement and change. In Australia, this has been recognised with the introduction of Aboriginal Community Controlled Health Services (ACCHS). First established in the 1970s, these services have improved engagement in health at a community level, contributed to improved health outcomes and increased clinic consultations. There is still somewhat fragmented and piecemeal funding of ACCHS, however, and further reform of Indigenous primary healthcare funding models is required.13
From 1998 to 2014 the overall Indigenous mortality rate has declined by 16%; however, there is still much more work needed to close the gap in life expectancy. To achieve targets, Indigenous life expectancy must increase at a faster rate than non-Indigenous life expectancy. It is expected that improved delivery of preventive care, primary care and acute care will be central, although it is also recognised that there is likely to be a time lag between commencement of key initiatives and improved outcomes. There has already been a sharp increase in Medicare benefits including chronic disease care plans and pharmaceuticals for chronic disease in Indigenous populations. There has been a small increase in the number of Indigenous people employed in healthcare services; however, this is still well below non-Indigenous rates.14
Important initiatives have been developed to improve the socioeconomic circumstances that will help drive better health outcomes, particularly in remote communities. These include policies and services to reduce violence and abuse of women and children, with stronger community policing. The introduction of cashless debit cards to reduce alcohol intake and gambling has been proposed, and collaborative approaches to improve nutrition through changes in pricing of healthy foods in remote community stores are becoming more widespread. Collaborations between Indigenous leaders and the Australian Federal Government will drive programs, including the recently announced $3.3 billion package for primary healthcare through the Indigenous Australians Health Programme. There is a further $85 million to improve culturally sensitive and appropriate mental healthcare through Primary Health Care Networks and $241 million for alcohol and drug treatment services. Remote housing and overcrowding is being addressed through a $5.5 billion program.14
Although it is likely that all of these measures will have considerable impact over time, to date there has been little evidence of progress, and there is a growing sense of urgency that more needs to be done. The initiatives that started 10 years ago will pave the way for a brighter future for young Indigenous people; however, a greater focus on efficient healthcare delivery, particularly for chronic disease management, is needed immediately. The very high prevalence of diabetes and its complications are overwhelming services, and primary care, particularly in remote settings, is often not adequately resourced to manage this. Although care planning is often used as a marker for good management of chronic disease, and supplies an income source for primary care, there is little evidence that it translates into improved outcomes, and in reality is a reward for measuring rather than acting on a patient’s progress. Improved clinic processes including reminder systems and patient registers, have been trialled in communities but these have had modest impact resulting in only short-term benefits.15
Innovative and collaborative treatment approaches are needed that will assist with improving outcomes in a population with a very high prevalence of chronic diseases and poor prognosis. Considerable thought and funding is needed to provide new evidence- based approaches to managing diabetes and other chronic diseases that will impact in the next five years to reduce the burden of complications. These approaches should include use of new therapies such as long-acting glucose lowering agents and lipid-lowering agents, and greatly increased chronic disease management workforce with associated capacity building for the Indigenous healthcare workforce.
Increasingly severe cardiac and renal diseases are seen in younger patients because of the burden of complications associated with young-onset and rapidly progressive type 2 diabetes. Those of us who visit remote communities understand the contribution of very poor glycaemic control to this growing problem. HbA1c readings of more than 15% (>140 mmol/mol) and random blood glucose levels above 30 mmol/L are common place, with onset of type 2 diabetes in children as young as 5 years old.16 There are a range of factors including housing, education, and availability and compliance of medications that contribute to such shocking outcomes; however, there is little doubt that diabetes both in Indigenous Australians and other Indigenous populations is aggressive and difficult to manage. Although there are no immediate solutions to these vast and complex issues, more support at a local level for over burdened primary care services must be a priority to impact on the preventable and devastating outcomes that we are increasingly seeing. Although government initiatives will improve many of the issues in the long term, it may be decades before an improvement in health outcomes is seen.
Summary
To close the gap in Australia, there is urgency for improved health outcomes in Aboriginal and Torres Strait Islander people, particularly focusing on chronic disease. This is an issue that is overwhelming healthcare services, and causing grave morbidity for many of our Indigenous people. The growing problem of diabetes in Indigenous people is a key contributor to the health and life expectancy gap that is, if anything, widening. The cause of the gap is multifactorial and complex, with links to poverty, remoteness, and low levels of health literacy and education. However, as in other Indigenous populations, there are strong genetic and epigenetic aspects to chronic diseases such as diabetes that drive poor outcomes. These are less well understood and appreciated by healthcare providers and payers, and there remains an unfortunate ‘shame and blame’ ideology that drives complacency and considers diabetes as predominantly a lifestyle illness.
Management of diabetes and other chronic diseases in Indigenous people requires new, aggressive and innovative management approaches, focusing on primary care resources and new therapies, to reduce the burden of complications and disability. To date there has not been enough progress in the management and prevention of chronic disease in the Indigenous population. As an immediate national health priority, focus groups are needed, involving government, Indigenous leaders and healthcare professionals, to develop improved efficiencies and resources for chronic disease healthcare delivery in Indigenous populations. ET
COMPETING INTERESTS: None.
References
- Australian Institute of Health and Welfare (AIHW). Australia’s Health 2014. Indigenous health 7.3 How healthy are Indigenous Australians? Canberra: AIHW, 2014. Available online at: www.aihw.gov.au/australias-health/2014/indigenous-health/#t3 (accessed March 2017).
- Ministry of Health. Mortality and demographic data 2012. Wellington: Ministry of Health; 2015. Available online at: www.health.govt.nz/publication/mortality-and-demographic-data-2012 (accessed March 2017).
- Indian Health Service (IHS). Trends in Indian health: 2014 Edition. Rockville:
- IHS, 2014.
- Australian Health Ministers’ Advisory Council, 2015, Aboriginal and Torres Strait Islander health performance framework 2014 Report, Canberra, AHMAC.
- Australian Institute of Health and Welfare: 2015. Aboriginal and Torres Strait Islander health performance framework 2012: detailed analyses. Cat. no.
- IHW 94. Canberra: AIHW; 2013.
- Australian Bureau of Statistics (ABS), Estimates of Aboriginal and Torres Strait Islander Australians, June 2011. Canberra: ABS; 2013.
- Neel JV. The ‘thrifty genotype’ in 1998. Nutr Rev 1999; 57(5 Pt 2): S2-S9.
- Naqshbandi M, Harris SB, Esler JG, Antwi-Nsiah F. Global complication rates of type 2 diabetes in Indigenous peoples: a comprehensive review. Diabetes Res Clin Pract 2008; 82: 1-17.
- Australian Institute of Health and Welfare (AIHW). Chronic kidney disease in Aboriginal and Torres Strait Islander people 2011. Cat. no. PHE 151 Canberra: AIHW; 2011.
- Hoy WE, Kincaid-Smith P, Hughson MD, et al. CKD in Aboriginal Australians. AMJ Kidney Dis 2010; 56: 983-993.
- Davis TM, McAullay D, Davis WA, Bruce DG. Characteristics and outcome of type 2 diabetes in urban Aboriginal people: the Fremantle Diabetes Study. Intern Med J 2007; 37: 59-63.
- Australian Bureau of Statistics (ABS). National Health Survey: First results, 2014-15 (4364.0.55.001). Canberra: ABS; 2015.
- Donato R, Segal L. Does Australia have the appropriate health reform agenda to close the gap in Indigenous health? Aust Health Rev 2013; 37
- 232-238.
- Australia Government Department of the Prime Minister and Cabinet.
- Closing the Gap – Prime Minister’s Report 2016. Canberra: Commonwealth of Australia; 2016. Available online at: http://apo.org.au/node/61524 (accessed March 2017).
- Forbes MP, Ling J, Jones S, McDermott R. Impacts and outcomes of diabetes care in a high risk remote indigenous community over time: Implications for practice. Aust J Prim Health 2013; 19: 107-112.
- Kevat D, Wilson D, Sinha A. A 5-year-old girl with type 2 diabetes. Lancet 2014; 383: 1268.