Falls and fractures in older people: identifying patients at high risk

Fractures
Falls are a major contributor to fractures in older people, yet most are preventable. A comprehensive risk-identification approach can help GPs identify older people at risk of falls and fractures and facilitate multidisciplinary, targeted intervention.
- The numbers of falls and fractures in Australia are increasing with the ageing of the population.
- GPs play a key role in assessing and treating patients at risk of falls and fractures.
- A falls risk assessment should be multifactorial.
- Osteoporosis should be considered in any patient over the age of 50 years with a previous fracture or risk factors.
- Useful tools are available for rapid assessment of falls and fracture risk.
- Interventions to reduce falls and fractures should be targeted and individualised.
Picture credit: © SilviaJansen/iStockphotos.com Model used for illustrative purposes only
Falls are a major contributor to fractures in older people, yet most are preventable. A comprehensive risk-identification approach can help GPs identify older people at risk of falls and fractures and facilitate multidisciplinary, targeted intervention.
Fragility fractures increase dramatically with advancing age, but bone mass does not show a comparable decline. This suggests that factors independent of bone loss contribute to the age-related increase in fracture risk. Falls appear a major contributor. For example, approximately 95% of hip fractures result from a fall, and fall risk factors such as prior falls and slow gait speed predict hip fracture independent of bone mineral density (BMD).
Most falls are preventable. GPs are pivotal in identifying and treating patients at risk of falls and fractures and facilitating a multidisciplinary approach to intervention. This article describes a comprehensive risk-identification approach for older patients at high risk that can facilitate intervention to help prevent both falls and fractures.
Epidemiology and consequences of falls in older people
About one-third of people over the age of 65 years living in the community have a fall each year.1 The risk of falls and fall-related injury increases with age.2 With the ageing of Australia’s population, falls and fall-related complications have increased despite increasing measures aimed at prevention.3
Falls result in significant morbidity and mortality.4 Most fall-related injuries are minor, such as bruising, lacerations, skin tears, strains and sprains. However, approximately 10% of falls result in fracture.5 About one-third of these fractures are of the hip and thigh, and many of these patients require extended hospitalisation and surgery.3 Falls may also result in avoidance of activities, social withdrawal, reduced quality of life, need for increasing care, including residential care, and death.6,7
Osteosarcopenia and the relation between falls and fractures
There is significant overlap between the risk factors for falls and those for fractures in older people. Muscle and bone are connected physically, chemically and metabolically.8 The term osteosarcopenia (the combination of osteopenia and sarcopenia) is applied to a subset of frailer individuals with both muscle and bone loss who are at higher risk of falls, fractures and subsequent complications.9 Although the concept of osteosarcopenia may seem complex, its recognition in patients serves multiple purposes. It contributes to the development of a patient risk profile and also indicates the need for treatment that addresses both muscle and bone deficiencies.
How to assess falls risk
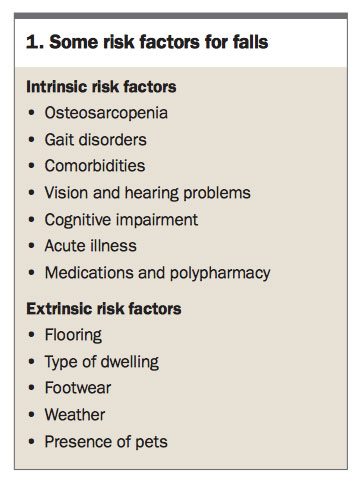
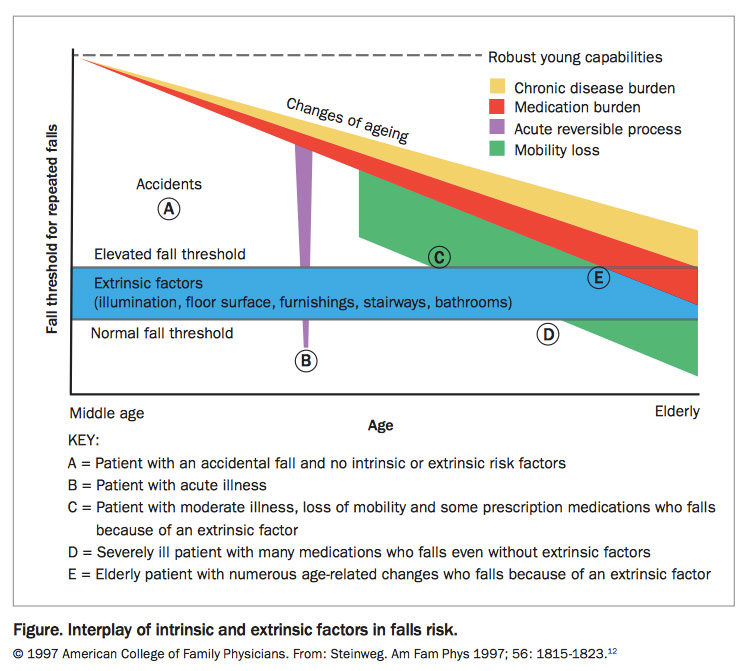
Most falls have multiple contributing factors, although a single major risk factor can be identified in about 20% of falls.10 Individual risk factors have a cumulative effect on total risk; the more risk factors a patient has then the higher is their risk of falls and fractures. The strongest risk factor for a fall is a previous fall.11 Most falls are caused by a combination of intrinsic and extrinsic factors (see Box 1 for examples).12 Individually and in combination, risk factors reduce the falling threshold (Figure).12
{kind=link}
{kind=link}
GPs should undertake a thorough falls risk assessment when any risk factor is identified, the likelihood of which increases with age. The presence of multiple risk factors suggests a patient is at high risk of falls, allowing clinicians to individualise their approach to the assessment of falls risk. Assessment should be multifactorial and include history taking, physical examination and investigations. Recommended investigations are discussed below in regard to fracture risk assessment. The approach to falls risk assessment differs between people in the community and those in residential care facilities.13 Given the time pressures faced by GPs, focusing on key risk factors as described below allows for an efficient, multifactorial assessment.
Importance of defining a fall
As the strongest risk factor for a fall is a previous fall, obtaining a clear history of any falls is vital.11 The concept of a ‘fall’ may seem quite obvious to clinicians, but patients may have a different understanding.14 Patients often focus on the consequences of falls and may not report events that have not led to injury. Clinicians should explain, using examples, that a fall is defined as any ‘unexpected event in which the person comes to rest on the ground, floor or lower level’.15 This would include events such as ‘slipping backwards’, even if this involved landing on an armchair.
History taking
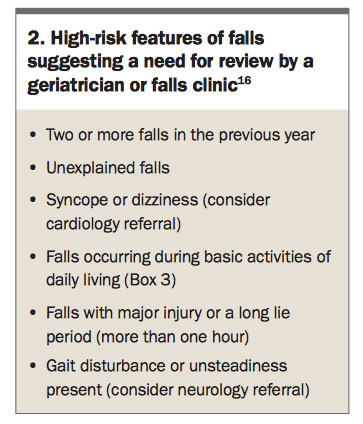
A sound history of any falls should enable the doctor to clearly re-create the individual setting and circumstances of the fall. A history from ‘significant others’ is often required to complement the history given by the patient. Some patients may not recall or may deny having a fall, in which case the collateral history becomes even more important. Whether the fall is related to presyncope or syncope should be determined, as this may warrant specific cardiac or neurological investigation and specialist referral. Other high-risk features suggesting the need for specialist review in community-dwelling adults with falls are listed in Box 2.16
{kind=link}
The history should also include information on comorbidities, medications, continence, vision and hearing impairment and cognition. Polypharmacy is a major risk factor for falls. Medications that independently increase the risk of falls include psychotropic medications, antidepressants and medications that increase the anticholinergic burden.17
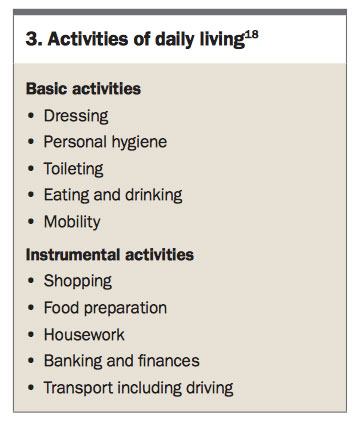
The social and functional history is a vital element of falls risk assessment. The patient’s function can be assessed through the activities of daily living (Box 3)18 or can be described in terms of personal, domestic and community activities of daily living.
{kind=link}
Physical examination
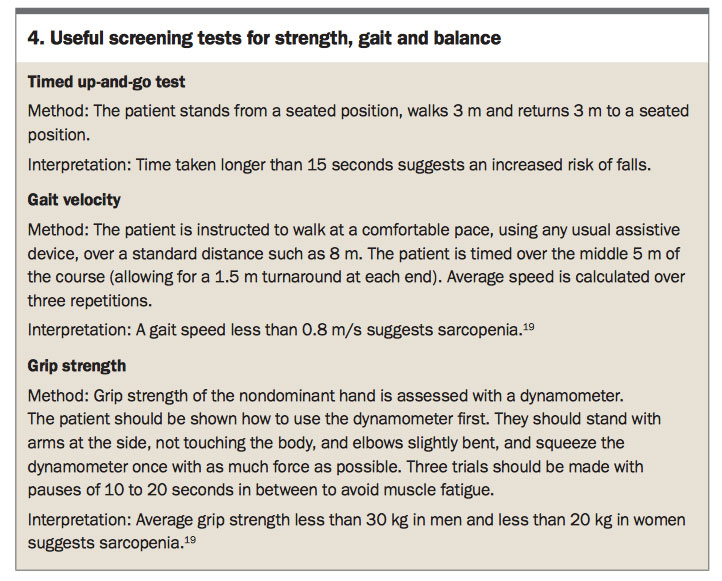
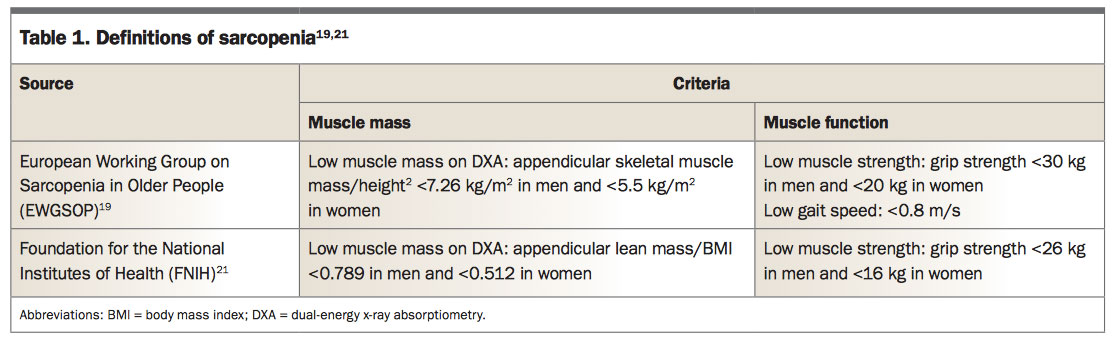
The physical examination should focus on identifying risk factors for falls. Useful screening tests for strength, gait and balance include the timed up-and-go test, gait velocity and grip strength (Box 4).19 Gait velocity is as useful as the timed up-and-go test in predicting most geriatric outcomes and tends to be more efficient.20 Gait velocity and grip strength measure muscle function and form part of the diagnostic criteria for sarcopenia, depending on the definition applied (Table 1).19,21 Sarcopenia, defined as the generalised, gradual loss of muscle mass, is an independent risk factor for falls and fractures.22
{kind=link}
{kind=link}
The short physical performance battery (SPPB) is another simple, validated test for assessing risk of falls and fractures.23 The SPPB examines the ability to stand with the feet together in the side-by-side, semi-tandem and tandem positions, time to walk 2 metres, and time to rise from a chair and return to the seated position five times.24
A neurological examination including assessment of visual acuity, hearing and peripheral sensation should be undertaken. If cognitive deficit is suspected then cognitive screening with a simple tool such as the Abbreviated Mental Test or the Standardised Mini-Mental State Examination should be considered. The feet and footwear should always be examined in the falls risk assessment, as abnormalities are often readily reversible.
How to assess fracture risk
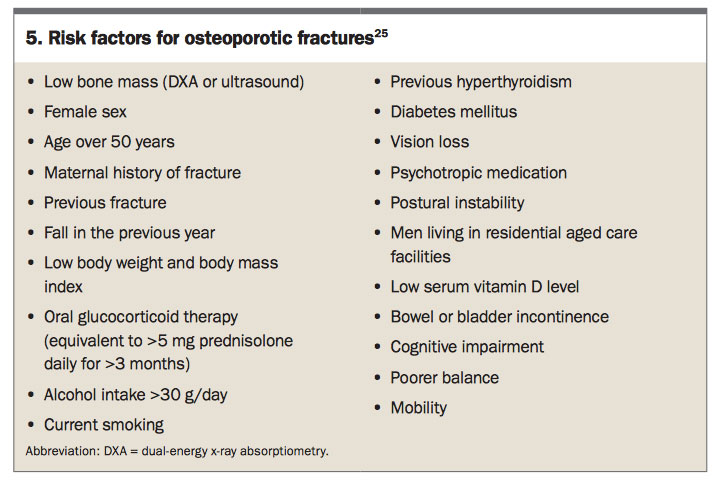
Given the relationship between falls, fractures and osteosarcopenia, it follows that patients at risk of falls are also at risk of fractures. The possibility of osteoporosis should be considered in all people over the age of 50 years. In addition, as 40% of all hip fractures occur in people living in residential care, a high index of suspicion for fracture risk should be applied to this population.13 Risk factors for osteoporotic fractures are listed in Box 5.25
{kind=link}
Fracture risk calculators
Simple, online tools that can help clinicians to identify and quantify fracture risk include the Fracture Risk Assessment Tool (FRAX; www.shef.ac.uk/FRAX) and the Garvan Fracture Risk Calculator (www.garvan.org.au/promotions/bone-fracture-risk/calculator). The Garvan tool was developed specifically for Australian GPs. One of these assessment tools should be applied to all patients suspected to be at risk of falls or fractures.
Dual-energy x-ray absorptiometry
Dual-energy x-ray absorptiometry (DXA) is the key investigation for determining BMD and fracture risk and diagnosing osteopenia and osteoporosis. It can also determine lean muscle mass, which is required for the diagnosis of sarcopenia.26
Osteoporosis is defined as a BMD that lies 2.5 standard deviations (SD) or more below the average value for young healthy women (T-score less than --2.5 SD) or a fracture due to low trauma.27 DXA should be repeated every two years in patients with established osteoporosis, and every two to five years in patients with osteopenia or those at high risk of osteoporosis, osteopenia or sarcopenia.28
How to investigate for secondary causes of falls and fractures
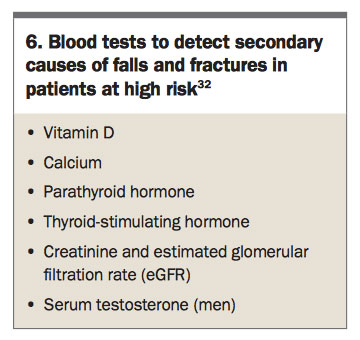
A variety of metabolic and endocrine disorders can increase the risk of falls and fractures.29,30 These disorders include vitamin D deficiency, hyperparathyroidism, hypothyroidism, hypogonadism and vitamin B12 and folate deficiency.30,31 These conditions may cause few or no symptoms or signs that point to the diagnosis, and thus screening investigations are recommended in patients at high risk of falls and fractures. Blood tests that can detect most secondary causes of falls and fractures are listed in Box 6.32 These tests should not be applied universally but rather focused on patients identified as being at high risk of falls and fractures.
{kind=link}
Management of patients with high falls or fracture risk
An evidence-based comprehensive care plan targeting all potential risk factors should be implemented for older patients with a high falls or fracture risk. The care plan should be individualised. Major components may aim to increase bone and muscle mass, improve muscle strength and function, prevent secondary causes of osteosarcopenia and reduce intrinsic and extrinsic risk factors for falls.
Interventions to reduce falls and fractures
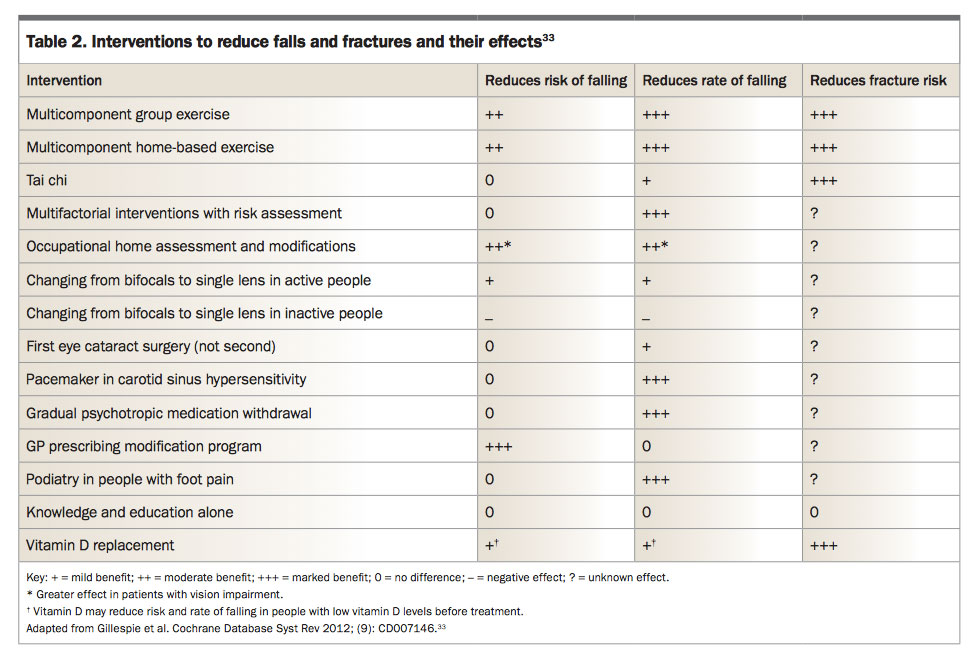
The most effective interventions targeting falls and fracture risk in older patients are individualised and multidisciplinary.33 Thorough history taking, physical examination and appropriate investigations should guide the development of a multidisciplinary program of interventions. Not all seemingly helpful interventions have been proven effective, and thus the program should be tailored to meet individual needs. In addition, interventions aiming to optimise independence, the perception of improved mobility and quality of life tend to be adopted more readily.34 The perception that one is ‘frail’ or a ‘faller’ can limit engagement with and adherence to interventions if they are not delivered in a manner acceptable to the patient.34 A range of interventions and their effects on falls and fracture risk are shown in Table 2.33
{kind=link}
Treatment of osteoporosis
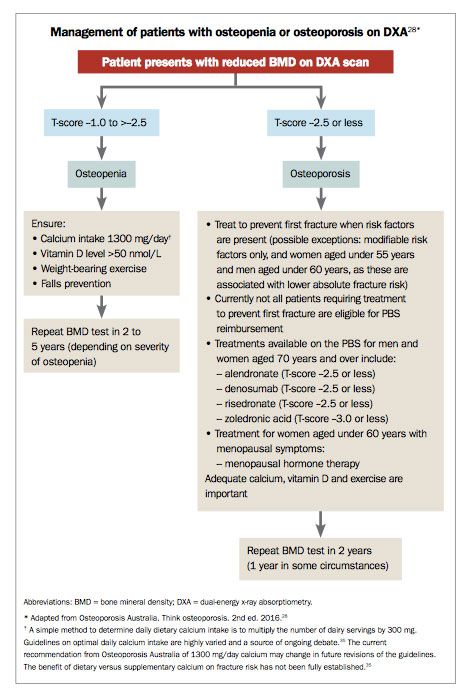
The RACGP together with Osteoporosis Australia have developed concise guidelines for the treatment of patients with osteoporosis. A review of the medical treatment of osteoporosis in older people is beyond the scope of this article. However, a useful guide for GPs that includes PBS information is available from Osteoporosis Australia (www.osteoporosis.org.au/sites/default/files/files/GP_Snap shot_2nd_Ed_07-16.pdf).28 Management actions, depending on the outcome of DXA, are outlined in the Flowchart.28,35
{kind=link}
Conclusion
The number of osteoporotic fractures has dramatically increased in the ageing Australian population. A significant number of high-risk patients are not being assessed for falls and fracture risk. A comprehensive multidimensional assessment of common and specific risk factors for falls and fractures is recommended. Clinical assessment should include a comprehensive physical examination and functional assessment (muscle strength, gait and balance). In addition, a DXA scan should be performed not only to quantify BMD but also to identify changes in body composition (osteosarcopenia). Finally, an evidence-based comprehensive care plan targeting all potential risk factors should be implemented on a case-by-case basis. ET
COMPETING INTERESTS: Professor Duque has received grants from Amgen and Novartis and serves as a member of a scientific advisory board for Amgen and Eli Lilly.
Dr Zanker: None.
References
- Campbell AJ, Borrie MJ, Spears GF, Jackson SL, Brown JS, Fitzgerald JL. Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study. Age Ageing 1990; 19: 136-141.
- Peel NM, Kassulke DJ, McClure RJ. Population based study of hospitalised fall related injuries in older people. Inj Prev 2002; 8: 280-283.
- Bradley C. Trends in hospitalisations due to falls by older people, Australia 1999-00 to 2010-11. Canberra: Australian Institute of Health and Welfare; 2013.
- Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip fractures.
- BMJ 1993; 307: 1248-1250.
- Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med 1988; 319: 1701-1707.
- Delbaere K, Crombez G, Vanderstraeten G, Willems T, Cambier D. Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. Age Ageing 2004; 33: 368-373.
- Yardley L, Smith H. A prospective study of the relationship between feared consequences of falling and avoidance of activity in community-living older people. Gerontologist 2002; 42:
17-23. - Levinger I, Phu S, Duque G. Sarcopenia and osteoporotic fractures. Clin Rev Bone Miner Metab 2016; 14: 38-44.
- Drey M, Sieber CC, Bertsch T, Bauer JM, Schmidmaier R; FiAT intervention group. Osteosarcopenia is more than sarcopenia and osteopenia alone. Aging Clin Exp Res 2016; 28: 895-899.
- Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospective study of people 70 years and older. J Gerontol 1989; 44: M112-M117.
- Deandrea S, Lucenteforte E, Bravi F, et al. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology 2010; 215: 658-668.
- Steinweg KK. The changing approach to falls in the elderly. Am Fam Physician 1997; 56: 1815-1823.
- Duque G, Lord SR, Mak J, et al. Treatment of osteoporosis in Australian residential aged care facilities: update on consensus recommendations for fracture prevention. J Am Med Dir Assoc 2016; 17: 852-859.
- Zecevic AA, Salmoni AW, Speechley M, Vandervoort AA. Defining a fall and reasons for falling: comparisons among the views of seniors, health care providers, and the research literature. Gerontologist 2006; 46: 367-376.
- Lamb SE, Jorstad-Stein EC, Hauer K, Becker C; Prevention of Falls Network Europe and Outcomes Consensus Group. Development of a common outcome data set for fall injury prevention trials: the Prevention of Falls Network Europe consensus. J Am Geriatr Soc 2005; 53: 1618-1622.
- Waldron N, Hill AM, Barker A. Falls prevention in older adults - assessment and management. Aust Fam Physician 2012; 41: 930-935.
- Park H, Satoh H, Miki A, et al. Medications associated with falls in older people: systematic review of publications from a recent 5-year period. Eur J Clin Pharmacol 2015; 71: 1429-1440.
- Auron-Gomez M, Michota F. Medical management of hip fracture. Clin Geriatr Med 2008; 24: 701-719, ix.
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al; European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010; 39: 412-423.
- Viccaro LJ, Perera S, Studenski SA. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J Am Geriatr Soc 2011; 59: 887-892.
- Studenski SA, Peters KW, Alley DE, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci 2014; 69: 547-558.
- Landi F, Liperoti R, Russo A, et al. Sarcopenia as a risk factor for falls in elderly individuals: results from the ilSIRENTE study. Clin Nutr 2012; 31: 652-658.
- Ward RE, Leveille SG, Beauchamp MK, et al. Functional performance as a predictor of injurious falls in older adults. J Am Geriatr Soc 2015; 63: 315-320.
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 1994; 49: M85-M94.
- Chen Y, Harrold LR, Yood RA, Field TS, Briesacher BA. Identifying patients with osteoporosis or at risk for osteoporotic fractures. Am J Manag Care 2012; 18: e61-e67.
- Bijlsma AY, Meskers MC, Molendijk M, et al. Diagnostic measures for sarcopenia and bone mineral density. Osteoporosis Int 2013; 24: 2681-2691.
- WHO. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. World Health Organization technical report series 843. Geneva: WHO; 1994. p. 1-129.
- Osteoporosis Australia. Think osteoporosis. 2nd ed. Sydney: Osteoporosis Australia; 2016.
- Tannenbaum C, Clark J, Schwartzman K, et al. Yield of laboratory testing to identify secondary contributors to osteoporosis in otherwise healthy women. J Clin Endocrinol Metab 2002; 87: 4431-4437.
- Hudec SM, Camacho PM. Secondary causes of osteoporosis. Endocr Pract 2013; 19: 120-128.
- Bours SP, van Geel TA, Geusens PP, et al. Contributors to secondary osteoporosis and metabolic bone diseases in patients presenting with a clinical fracture. J Clin Endocrinol Metab 2011; 96: 1360-1367.
- Johnson K, Suriyaarachchi P, Kakkat M, et al. Yield and cost-effectiveness of laboratory testing to identify metabolic contributors to falls and fractures in older persons. Archiv Osteopor 2015; 10: 226.
- Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 2012; (9): CD007146.
- Hill K, Vrantsidis F, Haralambous B, et al. An analysis of research on preventing falls and falls injury in older people: community, residential care and hospital settings. National Ageing Research Institute. Canberra: Australian Government; 2004.
- Bolland MJ, Leung W, Tai V, et al. Calcium intake and risk of fracture: systematic review. BMJ 2015; 351: h4580.